Translate this page into:
A rare developmental anomaly of the upper limb: Case of ulnar dimelia
2 College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia
Corresponding Author:
Majed N Alosaimi
Department of Surgery, Orthopedic Division, Ministry of the National Guard-Health Affairs, Jeddah; King Abdullah International Medical Research Center, Jeddah; King Saud bin Abdulaziz University for Health Sciences, Jeddah
Saudi Arabia
majedalosaimi@gmail.com
| How to cite this article: Alosaimi MN, Samman AT, Alswat MM, Alsaggaf KW. A rare developmental anomaly of the upper limb: Case of ulnar dimelia. J Musculoskelet Surg Res 2020;4:160-162 |
Abstract
Ulnar dimelia is a rare developmental anomaly, which is characterized by the duplication of ulna, absence of radius, and polydactyly. We report a case of a 5-year-old male child who was referred to our care with an extension deformity of the right elbow, loss of pronation and supination of the forearm, and flexion deformity with radial deviation of the ipsilateral wrist. Initially, we aimed to provide flexion of the elbow to improve his elbow function. The flexion was restricted to <10°. Intraoperatively, the posterior release of the capsule and the resection of the proximal part of the preaxial ulna allowed us to achieve 90° elbow flexion. A unique anatomic variation was a duplicate ulnar nerve on the lateral aspect, which was smaller than the normal ulnar nerve in the medial anatomical location. With three cases only being reported in Saudi Arabia and around 70 worldwide, each case is to be managed individually with a careful management plan.
Introduction
Ulnar dimelia, or known as mirror hand syndrome, is a rare congenital deformity of the upper limb with only three cases reported in Saudi Arabia and around 70 worldwide.[1],[2],[3],[4],[5],[6],[7] It is characterized by a duplication of the ulna, absence of the radius, and thumb with polydactyly (usually seven or eight digits). Apart from the skeletal deformity, there might be malformation of the arteries and nerves of the forearm, secondary to the skeletal deformities such as duplication of the ulnar nerve, duplication of the ulnar artery, or absence of the radial artery.[8] Ulnar dimelia is classified as the third group of congenital hand malformation, according to the Swanson classification.[8] Another classification of mirror hand deformity was proposed by Al-Qattan et al. based on the presence or absence of other congenital anomalies and the type of forearm bones present.[9] Its etiology has been attributed to the disturbance during embryonic development in zone of polarizing activity which controls the radioulnar development.[8],[10] The usual functional deficit with ulnar dimelia is reduced forearm and elbow motion.[11] In this paper, we aim to highlight the presentation and management of a rare pathology (a case of ulnar dimelia) that could be seen by pediatric orthopedic surgeons.
Case Presentation
A 5-year-old male child, not known to have any medical illness, presented to our clinic with a limitation of the right elbow flexion. He is a product of a full-term pregnancy. He has not been admitted to the neonatal intensive care. There was no history of consanguinity in the family. Moreover, there was no history of maternal use of medications, smoking, alcohol, or any illicit drugs. However, the mother was a passive smoker. He is the second among four healthy siblings with no history of congenital anomalies in the family.
Initially, at the age of 3 months, a skeletal survey was done by his pediatrician, which showed a right hand with seven digits, seven metacarpal bones, each with three phalanges, two extra numeric carpal bones, and two ulnas. The thumb and radius were not seen. He was referred to our pediatric orthopedic clinic for further evaluation.
On physical examination, he was a normal-appearing child, with no obvious deformities, going with the developmental growth according to his age. He had limited active abduction, forward flexion, and extension of the ipsilateral shoulder. The elbow showed full extension with 5°–10° of flexion with loss of pronation and supination of the forearm. The wrist joint showed wrist flexion contracture with radial deviation and seven digits with the absence of a thumb. The vascular examination was intact. He was diagnosed as a case of right ulnar dimelia. At the age of 20 and 33 months, radiographs were repeated and showed no growth arrest with the usual characteristic appearances. By the age of 4 years and 6 months, surgical intervention was performed, and a preoperative radiograph is shown in [Figure - 1]. He underwent resection of the proximal part of the preaxial ulna (lateral ulna) with soft tissue release under general anesthesia. The preoperative examination is shown in [Figure - 2].
![[Figure - 1]](#fig_SaudiOrthopJ_2020_4_3_160_281945_f1.jpg){kind=link}
![[Figure - 2]](#fig_SaudiOrthopJ_2020_4_3_160_281945_f2.jpg){kind=link}
 |
| Figure 1: Preoperative anteroposterior upper limp radiographs showing duplication of the ulna with seven metacarpal bones and seven digits |
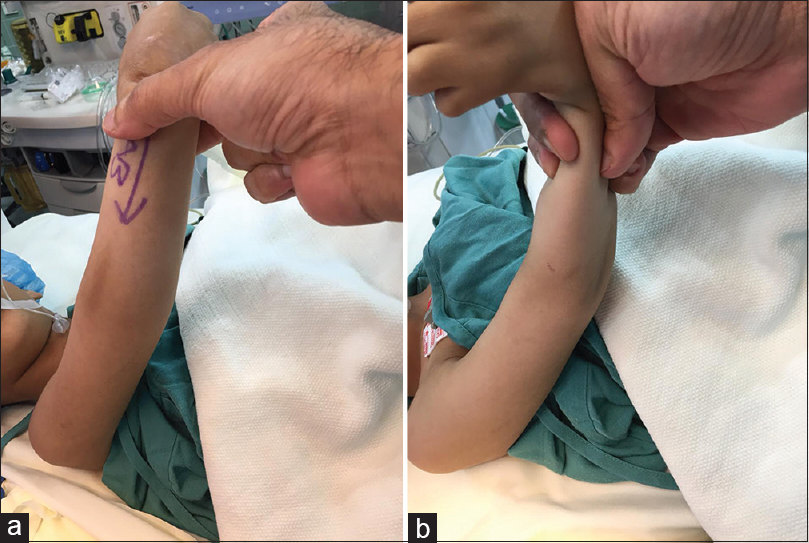 |
| Figure 2: (a) The elbow is in extension contracture with no passive flexion possible. (b) Passive flexion of the elbow showing a severe range of motion limitation (only 5°–10°) |
The aim of our surgical intervention was to achieve elbow flexion initially and to proceed, along with the help of plastic surgery's team, with the hand and wrist reconstruction in a consequent surgical setting.
Surgical procedure
Posterolateral longitudinal incision at the elbow was done. Dissection of the abnormal lateral epicondyle was performed. Triceps was found split into two halves, one half to the preaxial ulna and the other one to the postaxial. A lateral tunnel was noted, which contained what looked like a duplicate ulnar nerve on the lateral aspect. Medially, normal anatomy of the ulnar nerve, larger in size, twice as large as the lateral one was noted. The joint was opened posteriorly, and the range of motion improved after that by 5°–10° of flexion only, reaching 10°–20°. Posterior release of the capsule was done, the lateral collateral ligament was resected, while the medial collateral was preserved, and this allowed more flexion. Anterior release of the capsule was done proximally and helped us to gain another 40° of flexion. By resection of the proximal ulna on the lateral (preaxial) side, at the level of the coronoid process, we managed to have 90° flexion of the elbow. The distal humerus was in a three-lobed shape in the cross-section, the posterior lobe was the largest, maybe a condensation of two capitula together in the middle and posteriorly. Joint was unstable on the lateral area. The elbow was held in 90° flexion between the postaxial ulna and trochlea. The joint was fixed with two Kirschner (K) wires across the joint, which were passed percutaneously. Reconstruction of the lateral collateral ligament was done along with the approximation of the triceps tendon. Hemostasis was maintained, closure of the fascia was done in layers, and then the skin was closed. He tolerated the procedure well, and an above-elbow cast was applied. [Figure - 3] shows early postoperative radiographs. Six weeks postoperatively, K-wires were removed, and he was given an above elbow night splint in 90° of flexion. On 6-week, 3-month, and 6-month postoperative follow-up visits, he showed clinical healing of the surgical wound with a range of motion of 20°–80°. A 4-month postoperative radiograph is shown in [Figure - 4].
![[Figure - 3]](#fig_SaudiOrthopJ_2020_4_3_160_281945_f3.jpg){kind=link}
![[Figure - 4]](#fig_SaudiOrthopJ_2020_4_3_160_281945_f4.jpg){kind=link}
 |
| Figure 3: One-day postoperative radiographs |
 |
| Figure 4: Four-month postoperative radiographs |
Discussion
Our patient had two ulnas in the right forearm with seven digits, seven metacarpal bones each with three phalanges, two extra numeric carpal bones, and two ulnar nerves, and there was no thumb or radius. The two ulnas in our case were well formed, which lead us to classify our patient as type I-A, according to Al-Qattan et al. classification.[9] The goal of the management of such a condition is to improve upper limb function by performing single or multiple complex surgeries. In fact, multiple national such cases were managed differently. The management, in our case, was similar to a case that has been successfully managed by Al-Qattan et al. by excision of the olecranon of the preaxial (the lateral) ulna.[1] Another case that has also been managed by Al-Qattan et al. did not require any surgical procedure of the patient's elbow and achieved great improvement with physiotherapy only.[1] Furthermore, a third case managed by Rabah et al. by excision of part of the upper end of one of the ulnae resulted in an excellent outcome.[2]
However, shoulder, wrist, and elbow stiffness are the major problems in this disorder as they are difficult to manage and improve. On the other hand, pollicization and excess digits excision are successful in treating hand deformity.[2]
Conclusion
In cases of type I-A ulnar dimelia improving elbow, function is possible. We strongly advise doing flexion procedure to reposition the elbow in a functional position. Moreover, we do also advise to dissect carefully for the double ulnar nerve because it might be easily injured during the procedure.
Ethical considerations
Informed consent was signed by the parents, and institutional review board approval was obtained.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the child's parents have given their consent for images and other clinical information to be reported in the journal. The child's parents understand that his name and initials will not be published and due efforts will be made to conceal patient identity, but anonymity cannot be guaranteed.
Acknowledgments
We would like to thank the child's parents for approving reporting the case.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Authors' contributions
MNA has contributed with concepts, design, definition of intellectual content, manuscript preparation, editing, and review. ATS has contributed with concepts, definition of intellectual content, literature search, data acquisition manuscript preparation, editing, and review. MMA and KWA have contributed with design, literature search, data acquisition manuscript preparation, editing, and review. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
| 1. | Al-Qattan MM, Al-Kahtani AR, Al-Sharif EM, Al-Otaibi NJ. Thumb reconstruction without formal pollicization in mirror hand deformity: A series of four cases. J Hand Surg Eur Vol 2013;38:940-7. [Google Scholar] |
| 2. | Rabah S, Wani S. Mirror hand deformity—A rare congenital anomaly of the upper limb. Internet J Surg 2008;21:1-5. [Google Scholar] |
| 3. | Chinegwundoh JO, Gupta M, Scott WA. Ulnar dimelia. Is it a true duplication of the ulna? J Hand Surg Br 1997;22:77-9. [Google Scholar] |
| 4. | Gorriz G. Ulnar dimelia—A limb without anteroposterior differentiation. J Hand Surg Am 1982;7:466-9. [Google Scholar] |
| 5. | Afshar A. Ulnar dimelia without duplicated arterial anatomy. J Bone Joint Surg Br 2010;92:293-6. [Google Scholar] |
| 6. | Harpf C, Hussl H. A case of mirror hand deformity with a 17-year postoperative follow up. Case report. Scand J Plast Reconstr Surg Hand Surg 1999;33:329-33. [Google Scholar] |
| 7. | Gropper PT. Ulnar dimelia. J Hand Surg Am 1983;8:487-91. [Google Scholar] |
| 8. | Tomaszewski R, Bulandra A. Ulnar dimelia-diagnosis and management of a rare congenital anomaly of the upper limb. J Orthop 2015;12:S121-4. [Google Scholar] |
| 9. | Al-Qattan MM, Al-Thunayan A, de Cordier M, Nandagopal N, Pitkanen J. Classification of the mirror hand-multiple hand spectrum. J Hand Surg Br 1998;23:534-6. [Google Scholar] |
| 10. | Gaba S, John N, Bhogesha S, Singh O, Vemula GK. Mirror hand: An uncommon neglected case managed with pollicisation. World J Plast Surg 2017;6:263-5. [Google Scholar] |
| 11. | Cohen MH, Kozin S, Pederson W, Wolfe S, Green D. Deformities of the hand and fingers. In: Scott W, editors. Green's Operative Hand Surgery. 7th ed. Philadelphia: Elsevier, Inc.; 2017. p. 1237-8. [Google Scholar] |
Fulltext Views
2,192
PDF downloads
467




