Translate this page into:
Anterior transolecranon fracture-dislocation of the elbow in a 4-year-old child
Corresponding Author:
Alejandro Miravete-Galvez
ABC Medical Center, Mexico City
Mexico
dr.miravete@gmail.com
| How to cite this article: Miravete-Galvez A, Saleme-Cruz J, Jorba-Elguero P, Dabaghi-Richer A. Anterior transolecranon fracture-dislocation of the elbow in a 4-year-old child. J Musculoskelet Surg Res 2019;3:228-230 |
Abstract
Anterior elbow dislocation is a rare entity in the pediatric population, with only case reports or small series of cases found in the literature. Because of its extremely rare occurrence, there are low to nonexisting guidelines available for the correct and standardized treatment of this pathology. We present the case of a 4-year-old male who fell from a standing height, the exact mechanism of injury is unknown, and who sustained an anterior transolecranon fracture-dislocation of the left elbow. We performed a closed reduction of the fracture-dislocation, and fixation was made with one percutaneous 1.6-mm Kirschner wire, entering through the tip of the olecranon and anchoring the anterior cortex of the ulna. A posterior fiberglass elbow splint was placed for 1 week and changed to a fiberglass cast for 3 additional weeks. Five weeks after removing the fiberglass cast, the child's elbow motion was from 15° to 120°, with full pronation/supination, recovering full elbow motion at approximately 6 months. This case represents an extremely uncommon injury pattern, presenting as a potentially serious fracture-dislocation of the elbow; our results are a reminder of the importance of avoiding aggressive treatment modalities in young children, even in the presence of severely displaced articular injuries.Introduction
Anterior transolecranon fracture-dislocation is a well-known entity in skeletally mature patients, with prevalence and mechanism of injury clearly elucidated.[1],[2] In the pediatric population, the mechanism is believed to be one of the hyperextensions, with the olecranon making a fulcrum with the olecranon fossa pushing anteriorly the most proximal portion of the ulna and leaving the tip of the olecranon posteriorly, which is pulled back/proximally by the insertion of the triceps tendon.[3]
The exact prevalence of this lesion is difficult to know due to only case reports or small series of cases being found in the literature.[1],[3],[4],[5] In a study made between 1994 and 2002, Rasool reviewed a series of 33 elbow dislocations in children: 30 dislocations were posterior and only three were anterior.[4] Since 1785 when it was first described, approximately only 70 cases of anterior elbow dislocation in children have been reported in the English literature and the majority of them are associated with a transolecranon fracture.[3],[6],[7]
Because of its extremely rare occurrence, there are low to non-existing guidelines available for the correct and standardized treatment of this pathology.
The purpose of this report is to show a successful treatment strategy for this extremely rare injury, for which no guidelines are available in the existent scientific literature.
Case Report
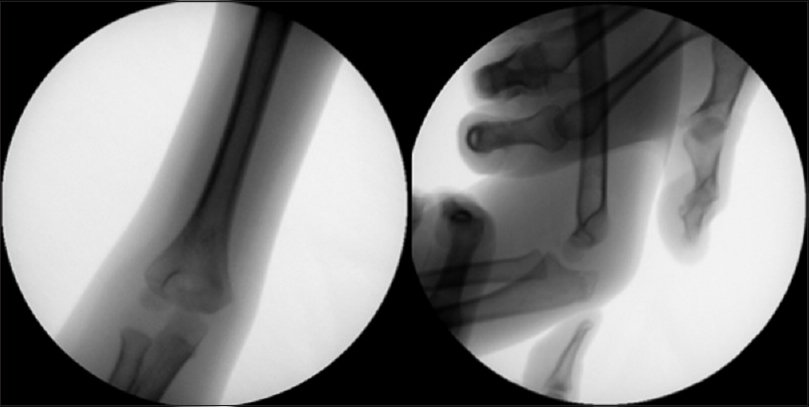
We present the case of a 4-year-old male who fell from his own height; the exact mechanism of injury is unknown. He sustained an anterior transolecranon fracture-dislocation of the left elbow [Figure - 1]. The child presented to the emergency room with extreme pain and obvious deformity of the elbow. After pain relief medication, a thorough neurovascular examination was made, which encountered no abnormalities.
![[Figure - 1]](#fig_SaudiOrthopJ_2019_3_2_228_252782_f1.jpg){kind=link}
 |
| Figure 1: Anterior–posterior and lateral X-ray films of the left elbow, showing an anterior transolecranon fracture dislocation |
The patient had not yet developed an olecranon secondary ossification center, and the olecranon fracture occurred distal to the olecranon apophysis [Figure - 1].
The child was taken to the operating room 1 h after his arrival to the emergency room, and he was placed in a decubitus supine position with the left elbow over the image receptor of the fluoroscope.
Closed reduction of the fracture-dislocation was then made by applying firm axial traction, elbow flexion, and sustained pressure over the tip of the olecranon, achieving clinical correction of the deformity. The correct reduction was then confirmed with fluoroscopic images [Figure - 2].
![[Figure - 2]](#fig_SaudiOrthopJ_2019_3_2_228_252782_f2.jpg){kind=link}
 |
| Figure 2: Anterior–posterior and lateral fluoroscope images showing successful reduction of fracture luxation |
Fixation of the olecranon was made with one percutaneous 1.6-mm Kirschner wire entering the tip of the olecranon and anchored to the anterior cortex of the ulna. Stability of the fixation was then tested through both elbows and forearm complete range of motion [Figure - 3].
![[Figure - 3]](#fig_SaudiOrthopJ_2019_3_2_228_252782_f3.jpg){kind=link}
 |
| Figure 3: Fixations with one percutaneous Kirschner wire 1.6 mm entering the tip of the olecranon and anchored to de anterior cortex of the ulna |
A posterior fiberglass elbow splint at 90° of flexion and neutral position of the forearm was placed for 1 week and changed to a full fiberglass cast (same position) for 3 additional weeks.
The Kirschner wire was removed after 4 weeks when radiographic evidence of adequate consolidation and articular congruency was observed [Figure - 4].
![[Figure - 4]](#fig_SaudiOrthopJ_2019_3_2_228_252782_f4.jpg){kind=link}
 |
| Figure 4: Four weeks follow-up anterior–posterior and lateral X-rays with excellent consolidation a good articular congruency |
Five weeks after removing the fiberglass cast, the child's elbow motion was from 15° to 120°, with full pronation/supination [Figure - 5] and [Figure - 6].
![[Figure - 5]](#fig_SaudiOrthopJ_2019_3_2_228_252782_f5.jpg){kind=link}
![[Figure - 6]](#fig_SaudiOrthopJ_2019_3_2_228_252782_f6.jpg){kind=link}
 |
| Figure 5: Five-week clinical images, demonstrating almost full extension and 120° of flexion |
 |
| Figure 6: Five-week clinical image, showing full pronation and no neurovascular impairment |
In the last follow-up visit made 6 months after the surgery, the elbow's range of motion had recovered to full extension [Figure - 7].
![[Figure - 7]](#fig_SaudiOrthopJ_2019_3_2_228_252782_f7.jpg){kind=link}
 |
| Figure 7: Six-month follow-up demonstrating full extension and 120° of flexion |
Discussion
There is little information in the scientific literature regarding the correct management of this type of injuries; some low-grade evidence recommendations can be found. For example, Butler et al. studied the results of three pediatric variants of anterior transolecranon fracture-dislocations, treated with tension band construct, reporting excellent results.[1] In another study by Guitton et al., they suggested that since tension band alone is well known to be insufficient in adults with this type of fracture, it should be assumed that this would also be the case for children. Hence, they suggested that plate fixation would be a better treatment option; however, this report included only three cases, all of which were more skeletally mature than our patient (8–11 years old).[8]
Whereas some may argue that our osteosynthesis is insufficient, the good results seen in this case are unquestionable, with the patient's range of motion being almost complete at 5 weeks after removal of the cast, with radiographs showing excellent consolidation and articular congruency. One advantage of our approach is that since closed reduction and fixation were done, the fracture hematoma and soft tissues were respected, which may also have contributed to the good outcome.
This case represents an extremely uncommon injury pattern, presenting as a potentially serious fracture-dislocation of the elbow, with a high risk of neurovascular compromise, as well as a pattern of displacement that suggests significant injury to the capsuloligamentous structures of the elbow. Our patient's excellent post-operative outcome is remarkable in view of this, particularly when considering the minimal nature of the surgical treatment that was performed. In spite of a theoretically unstable fixation, with only one pin in the olecranon, and the lack of any attempt at repairing ligaments and the joint capsule, the patient regained a complete range of motion, without any neurovascular damage. Although this is a single-case report, we believe that the excellent results observed in this case can serve as a reminder of the importance of avoiding aggressive treatment modalities in young children, even in the presence of severely displaced articular injuries, regardless of the particular injury pattern.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Author's contributions
AMG, JSC, PJE, ADR conducted research and provided research materials, AMG and PJE wrote initial and final draft. JSC provided photos and follow up information. JSC, PJE and ADR revised the article and contribute important intellectual content. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
| 1. | Butler MA, Martus JE, Schoenecker JG. Pediatric variants of the transolecranon fracture dislocation: Recognition and tension band fixation: Report of 3 cases. J Hand Surg Am 2012;37:999-1002. [Google Scholar] |
| 2. | Ring D, Jupiter JB, Sanders RW, Mast J, Simpson NS. Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-50. [Google Scholar] |
| 3. | Wilkerson RD. Anterior elbow dislocation associated with olecranon fractures – Review of the literature and case report. Iowa Orthop J 1993;13:223-5. [Google Scholar] |
| 4. | Rasool MN. Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-8. [Google Scholar] |
| 5. | Bouaziz W, Guidara AR, Trabelsi A, Bardaa T, Hammami M, Ellouz Z, et al. Anterior transolecranon dislocation of the elbow in a child: A case report and review of literature. World J Orthop 2018;9:100-4. [Google Scholar] |
| 6. | Suzuki T, Yoshida H, Matsumura N, Iwamoto T, Ochi K, Sato K. Anterior transverse divergent dislocation of the elbow in a child: A case report. JBJS Case Connect 2015;5:e75. [Google Scholar] |
| 7. | Kumar R, Sekhawat V, Sankhala SS, Bijarnia I. Anterior dislocation of elbow joint-case report of a rare injury. J Orthop Case Rep 2014;4:16-8. [Google Scholar] |
| 8. | Guitton TG, Albers RG, Ring D. Anterior olecranon fracture-dislocations of the elbow in children. A report of four cases. J Bone Joint Surg Am 2009;91:1487-90. [Google Scholar] |
Fulltext Views
2,210
PDF downloads
1,110




