Translate this page into:
Assessment of knowledge and awareness regarding radiation safety and fluoroscopy use among orthopedic surgeons in Saudi Arabia
2 Department of Orthopedic Surgery, Al Noor Specialist Hospital, Makkah, Saudi Arabia
3 College of Medicine, Taif University, Taif, Saudi Arabia
Corresponding Author:
Hashem A Bukhary
Department of Surgery, Division of Orthopedic, College of Medicine, Taif University, Taif
Saudi Arabia
h.abdulrahim@tu.edu.sa
| How to cite this article: Bukhary HA, Aldosari AM, Althagafi AS. Assessment of knowledge and awareness regarding radiation safety and fluoroscopy use among orthopedic surgeons in Saudi Arabia. J Musculoskelet Surg Res 2021;5:35-40 |
Abstract
Objectives: Orthopedic surgeons are heavy fluoroscopy users, which is one of the primary sources of ionizing radiation. Therefore, risks from exposure to these radiations need to be appraised. This study aimed to estimate orthopedic surgeons' knowledge and awareness in Saudi Arabia regarding radiation safety and fluoroscopy use. Methods: This cross-sectional study was conducted from May to August 2020. A total of 150 replies were received from various cities in Saudi Arabia to an 18-item questionnaire. It covered frequency of radiation exposure, safety measures used, and training for radiation safety and fluoroscopy use. Results: The study showed a broad unfortunate negative-associated trend in surgeons' knowledge, with the training of radiation safety and fluoroscopy use, especially for eye and hand-related safety precautions. However, 61% of male surgeons and 48.6% of female surgeons were significantly worried about diseases caused by radiation exposure. Conclusion: This study revealed that most orthopedic surgeons in Saudi Arabia have a limited background on ionizing radiation risks and safe fluoroscopy use. Awareness of radiation safety is required for the well-being of orthopedic surgeons.
Introduction
Radiation imaging is a useful fundamental tool in many surgical procedures; however, exposure to ionizing radiation is hazardous and could be deadly for humans.[1] Operative fracture fixation employs fluoroscopy imaging making orthopedic surgeons operating on trauma or deformity surgeries more susceptible to radiation risks.[1],[2],[3]
Knowledge about radiation and safety protection among orthopedic surgeons is lacking, despite the high dependence on fluoroscopy in their practice.[4],[5] According to the current guidelines of the National Council on Radiation Protection and Measurements, based on the radiation protection guidelines of the International Commission on Radiological Protection (ICRP), the main approach to directly decrease ionizing radiation exposure involves keeping exposure as low as reasonably achievable (ALARA). Besides, confirming the total benefit of fluoroscopy to surgery and keeping the annual danger of exposure within dose limits. These guidelines are for reducing the quantity of radiation exposure to both the expert personnel and individuals.[6],[7]
Surgeons should be aware of the dangers associated with ionizing radiation examination.
Harmful malignant effects of ionizing radiation, as research has shown, can cause most forms of cancer. Thyroid, breast, and lung cancer, along with bone marrow dysplasia, are most susceptible to initiation by these harmful radiations.[8] Thyroid cancer risk is exceptionally high among orthopedic surgeons.[9] In addition, nonmalignant adverse effects on the eyes, gonads, and skin were reported with ionizing radiation. These include cataract, infertility, and skin changes, respectively.[1],[10]
All estimated dangers, even modest ones, are unacceptable if they do not benefit the patient.[11] To our knowledge, no study on orthopedic surgeons in Saudi Arabia has measured the awareness level of fluoroscopy use and radiation safety during surgery. Thus, this study aimed to evaluate their knowledge and awareness of radiation exposure safety during fluoroscopy use.
Subjects and Methods
A cross-sectional study was conducted from May to August 2020 to evaluate orthopedic surgeons' behavior and knowledge skill in Saudi Arabia regarding radiation safety and fluoroscopy use.
The inquiry of this survey was adapted from a published study (with permission).[5] An anonymous, 18-item questionnaire covered the frequency of radiation exposure, safety measures used, and training for radiation safety and fluoroscopy use; the questionnaire was created on Google Forms.
The questionnaire included specific behavioral radiation safety assessment with one possible answer question. Furthermore, the question about the utilization of shielding gear while using fluoroscopy, as designed, had more than one answer. The content of the questionnaire is detailed in Appendix 1. Estimating around 3000 orthopedic surgeons are practicing in Saudi Arabia at this period. The sample size needed was calculated as 249 based on the following formula: sample size = ([z-score]2[population proportion] [1-population proportion])/(margin of error%)2. The link was sent through personal phone messages to 340 orthopedic surgeons living in Saudi Arabia with another reminder message sent 4 weeks after the initial one. All completed online questionnaires were collected on an Excel Spreadsheet and exported to the Statistical Package for the Social Sciences (SPSS) file.
Data were analyzed using the SPSS software version 21.0 (IBM Corp, Armonk, NY, USA). Frequencies and percentages were used for each variable. The Chi-square test was used to study the relationship between variables, and the t-test was used for comparison between means. A P ≤ 0.05 was considered statistically significant.
Results
Only 150 random orthopedic surgeons, out of the 340, answered the questionnaire. The response rate was 44.1% of those who got the survey. Among them, 133 (75.3%) surgeons were males and 37 (24.7%) were females. The percentage of participants from each region is presented in [Figure - 1]. One hundred and forty-six (97%) surgeons of the total participants were exposed to fluoroscopic radiation at least once a week or more. In contrast, four (3%) were exposed once a month. Ninety-six (64%) responders were residents, 32 (22%) were specialists, and 22 (14%) were consultants. One hundred and twenty-seven (84.7%) surgeons were from government hospitals, 14 (9.3%) were from university hospitals, and 9 (6%) were from private hospitals.
![[Figure - 1]](#fig_SaudiOrthopJ_2021_5_1_35_299953_f1.jpg){kind=link}
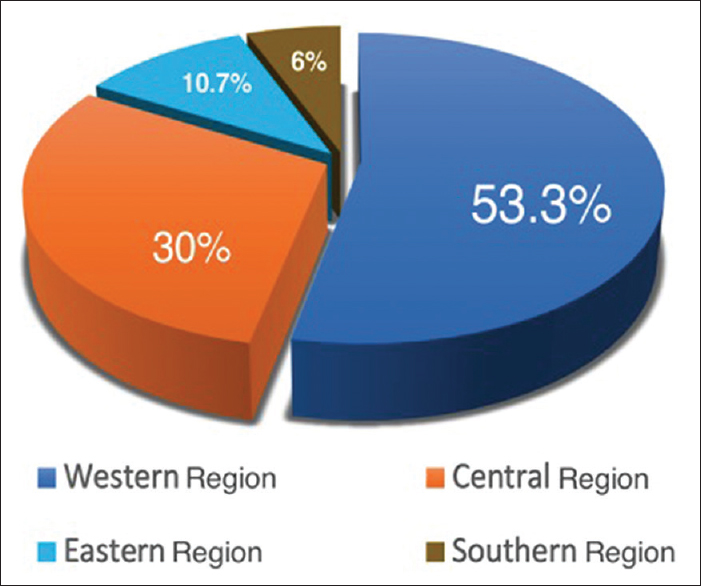 |
| Figure 1: Surgeons' distribution according to the region in Saudi Arabia |
When participants were asked whether or not they worried about the safety of ionizing radiation, surgeons were significantly worried (P = 0.041) [Table - 1]. In contrast, when participants were asked whether or not they feel secure about using fluoroscopy, approximately 76% of the surgeons did not feel secure compared to the 24% who were feeling secure. Seventy-seven (80.2%) residents, 23 (69.7%) specialists, and 14 (66.7%) consultants were not feeling secure about fluoroscopy usage and radiation exposure. A comparison of fluoroscopy usage insecurity according to participant's professional rank was insignificant (P = 0.265).
![[Table - 1]](#tbl_SaudiOrthopJ_2021_5_1_35_299953_t3.jpg){kind=link}

The number of consultants, specialists, and residents who were not trained on fluoroscopy usage was higher and statistically significant (P = 0.016) when compared to their professional ranks. Moreover, the number of surgeons who were not trained on fluoroscopy usage was also higher but statistically not significant (P = 0.117) when compared to their gender [Table - 2]. Furthermore, most of the surgeons (87.3%) were not trained in radiation safety. One hundred and eleven worked at governmental hospitals, 13 at university hospitals, and 7 at private hospitals. When the answers related to radiation safety training were compared with their working hospitals, there was no remarkable difference (P = 0.568). In addition, when the results related to radiation safety training were compared with surgeons' gender, there was marginal significance (P = 0.059) [Table - 3].
![[Table - 2]](#tbl_SaudiOrthopJ_2021_5_1_35_299953_t4.jpg){kind=link}
![[Table - 3]](#tbl_SaudiOrthopJ_2021_5_1_35_299953_t5.jpg){kind=link}


When asked about the protective equipment, all participants used at least one form of protection. The lead aprons were the most frequently selected (149; 98.7%) by participants; 60 (40%) selected thyroid shields, and only five (3.3%) of them wore radioprotective glasses. Interestingly, no one used radioprotective gloves [Table - 4]. When the use of protective equipment was compared in terms of gender, there was no significant difference (P = 0.66). Regarding the safety sign on the operating room door, 119 (79.3%) said they do not use a sign on the operation room door when fluoroscopy is used, and 31 (20.7%) said they use a sign.
![[Table - 4]](#tbl_SaudiOrthopJ_2021_5_1_35_299953_t6.jpg){kind=link}

Moreover, while wearing the equipment, the outcome of this questionnaire showed that only 25 (16.7%) of the responders stood at least 2 m away; 81 (45%) stood 1–2 steps while wearing the equipment; and 44 (29.3%) did not pay attention to the distance. There was no significant difference between the professional rank and where responders stood (P = 0.093).
In the present study, 44 (29.3%) orthopedic surgeons said that the C-arm position did not make a difference to them. Sixty-one (40.7%) surgeons chose that the C-arm device was positioned as the X-ray tube (source) at the bottom and the X-ray receiver at the top, while 45 (30%) said that the C-arm was positioned with the X-ray receiver at the bottom and the X-ray tube (source) at the top. There was no significant difference when we compared these data to their professional rank (P = 0.442).
Only 86 (57.3%) surgeons utilize radiology technician's assistant. In contrast, 64 (42.7%) surgeons obtain aid from either the operating room staff or anyone directed by the surgeon for fluoroscopy use. Although a dosimeter is essential to measure the dose of annual exposure, we found that it was rarely used in this study. Therefore, the surgeons had no reliable data to calculate the average yearly risk of radiation exposure.
Discussion
Regardless of their professional rank, orthopedic deformity and trauma surgeons are exposed to a remarkable risk of ionizing radiation, as opposed to other specialties.[3] Even with the expansion of mini fluoroscopy (mini C-arm), significant radiation exposure to the surgeon can occur. Therefore, this will require reiteration of radiation safety awareness among orthopedic surgeons.[12] The analysis in this study took into account the experience of surgeons, along with their working hospitals. Moreover, the awareness regarding the main ALARA principles was also considered in the study. Even with a little dose of radiation, ALARA principles state that measures of safety must decrease the dose by adjusting time, distance, and shielding elements.[6] After interpreting the data, many orthopedic surgeons in Saudi Arabia were unexpectedly found to lack awareness and practice regarding ionizing radiation risks. Unfortunately, the absence of a radiation safety instruction course during residency years could be the reason for the lack of awareness.[6]
The harmful effects of ionizing radiation are manifested at the cellular level, which develops the risk of cancer and other diseases. This insult can happen either through energy causing direct nuclear damage of the cell nuclear formation or through an indirect ionizing effect where water turns into free radicals.[1],[6],[8],[10] In this study, 61% of the male surgeons and 48.6% of the female surgeons were substantially worried about these diseases.
Embracing the ALARA principles, by utilizing protective equipment, distancing the radiation source, and lowering ionizing radiation exposure dose will reduce the radiation danger.[1],[6] Using the thyroid shield offers a significant decrease in radiation danger to the thyroid gland and its surroundings and can reduce it to background levels.[9] Thyroid shield was used by only 40% of participants in this study. A protective apron, which has not been worn out, will absorb over 90% of the scattered radiation with a lead-equivalent thickness of at least 0.5 mm.[2],[6] The protective apron was used by almost all surgeons (98.6%). A decline of radiation exposure, ranging from 8 to 22 times to the surgeon's eyes, is expected with the use of radioprotective glasses.[13] However, only 3.3% were using radioprotective glasses. Furthermore, using radioprotective gloves can be used to attenuate the radiation to the hand.[6] In this study, it was observed that no one was using radioprotective gloves. However, it is easier to keep hands out of the radiation field.[6]
In the present study, only 16.7% stood at more than 2 m distance from the C-arm while using it. According to literature, increasing the distance from the radiation device, following the inverse-square law, will subsequently lower the dose reaching the surroundings. Hence, staying more than 2 m away will safely reduce exposure.[1],[2],[6]
If the C-arm position is with the source (the tube) on the top of the table, it will create more scatter radiation for the surgeon. Therefore, it is preferable for the C-arm tube to be placed below the table.[1],[2],[6] In the current study, it was found that only 30% of participants were placing the radiation source below the table [Figure - 2]. In comparison, 70% of participants were found to be unaware of the risk with the position of the source.
![[Figure - 2]](#fig_SaudiOrthopJ_2021_5_1_35_299953_f2.jpg){kind=link}
 |
| Figure 2: The preferable setup with the X-ray tube (arrow) on the bottom |
Since the radiation protection principle of ICRP is to lower ionizing radiation exposure time, establishing a mutual connection with the operator will lower the time and limits its danger.[6],[7],[10] In the present study, only 57.3% of the surgeons utilized a radiology technician's assistant. In the case that an unqualified operator is sought, the risk will increase significantly.
Some limitations of this research deserve mentioning. One limitation was related to its sample size compared to the total orthopedic surgeons in Saudi Arabia. In addition, the electronically distributed questionnaire generated a low response rate. Questions on the usage of a dosimeter and it is annual dose check were asked; however, the collected results were unsatisfactory. Moreover, when a question was presented on safety equipment, we failed to ask if surgeons checked on the quality of the apron. These limitations can be overcome in future studies by increasing the sample size. The strength of this survey is that it is one of the rare studies conducted in Saudi Arabia, aiming to evaluate orthopedic surgeons' awareness about fluoroscopy ionizing radiation. Besides, the survey was comprehensive as it included multiple regions within Saudi Arabia.
Conclusion
This research revealed that most orthopedic surgeons in Saudi Arabia have limited background on ionizing radiation risks, especially eye and hand-related risks; therefore, they need to stay aware and practice safety.
Recommendations
All trainers should be aware of fluoroscopy radiation and its dangers. Moreover, radiation danger can be minimized by carefully following the ALARA principles. A future study to evaluate the patients' safety measures regarding radiation is also suggested. Also, to include the subject in the postgraduate curriculum of orthopedic specialties.
Acknowledgment
The authors are extremely grateful to all the associated personnel that contributed to this study. Further, the authors appreciate support from the Research Ethics Committee of Scientific Research Deanship at Taif University.
Ethical consideration
Ethical approval was obtained from the Research Ethics Committee of Taif University (Approval # 41-00169, May 07, 2020). No names were inquired. Further, all participants were informed and agreed to participate and get their results published.
Financial support and sponsorship
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
There are no conflicts of interest.
Authors' contributions
HAB has contributed to conception, design, definition of intellectual content, literature search, formal analysis, manuscript preparation and editing. AMA has contributed to conception, definition of intellectual content, literature search, data acquisition manuscript preparation and editing. ASA contributed to conception, literature search, formal analysis, data acquisition manuscript preparation and editing. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Appendix
Appendix 1: Questionnaire distributed
- What is your professional rank?
- Which region do you work in?
- Gender
- Which institution do you work for?
- How often are you exposed to fluoroscopic radiation?
- Have you been trained to use fluoroscopy?
- Do you feel secure about fluoroscopy use and radiation exposure?
- Do you use any protective equipment? (More than one answer is applicable)
- Do you ever have protective equipment checked for effectiveness or expiration?
- Do you use a dosimeter for exposure?
- If you are using a dosimeter, do you routinely send it for measurements?
- Is the radiation safety of the operating room taken?
- Are there any warning signs on the door of the rooms when the fluoroscopy is used?
- Are you worried about radiation exposure?
- Who uses the fluoroscope in the operating room?
- How far away from the device do you stay during fluoroscopy use while wearing your protective equipment?
- At which position does the C-arm device stand during use?
- Have you been trained for radiation safety?
o Consultant
o Specialist
o Resident.
o Central
o Western
o Eastern
o Southern.
o Female
o Male.
o University hospital
o Governmental training hospital
o Private hospitals.
o Once a month
o Once a week
o 2–5 times a week
o 6 or more times a week.
o Yes
o No.
o Yes
o No.
o The protective apron
o Radioprotective glasses
o Radioprotective gloves
o Thyroid shields.
o I do not use any.
o Yes
o No
o I do not know.
o Yes
o No.
o Yes
o No
o I do not know.
o Yes
o No
o I do not know.
o Yes
o No
o I do not know.
o Yes
o No
o Sometimes.
o Radiology technicians only
o Operating room staff
o Anyone directed by the surgeon.
o 1–2 steps
o At least 3M
o I do not care.
o The X-ray tube (source) at the bottom, the X-ray receiver at the top
o The X-ray receiver at the bottom, the X-ray tube (source) at the top
o I do not care.
o Yes
o No.
| 1. | Dewey P, George S, Gray A. Ionising radiation and orthopaedics. Curr Orthop 2005;19:1-12. [Google Scholar] |
| 2. | Giordano BD, Grauer JN, Miller CP, Morgan TL, Rechtine GR 2nd. Radiation exposure issues in orthopaedics. J Bone Joint Surg Am 2011;93:e69. [Google Scholar] |
| 3. | Gausden EB, Christ AB, Zeldin R, Lane JM, McCarthy MM. Tracking cumulative radiation exposure in orthopaedic surgeons and residents: What dose are we getting? J Bone Joint Surg Am 2017;99:1324-9. [Google Scholar] |
| 4. | Khan F, Ul-Abadin Z, Rauf S, Javed A. Awareness and attitudes amongst basic surgical trainees regarding radiation in orthopaedic trauma surgery. Biomed Imaging Interv J 2010;6:e25. [Google Scholar] |
| 5. | Fidan F, Çetin MÜ, Kazdal C, Kılıç F, Özkaya U. Behaviour and knowledge skill levels of orthopedic surgeons about radiation safety and fluoroscopy use: A survey analysis. Acta Orthop Traumatol Turc 2019;53:301-5. [Google Scholar] |
| 6. | Kaplan DJ, Patel JN, Liporace FA, Yoon RS. Intraoperative radiation safety in orthopaedics: A review of the ALARA (as low as reasonably achievable) principle. Patient Saf Surg 2016;10:27. [Google Scholar] |
| 7. | Kase KR. Radiation protection principles of NCRP. Health Phys 2004;87:251-7. [Google Scholar] |
| 8. | Wakeford R. The cancer epidemiology of radiation. Oncogene 2004;23:6404-28. [Google Scholar] |
| 9. | Tse V, Lising J, Khadra M, Chiam Q, Nugent R, Yeaman L, et al. Radiation exposure during fluoroscopy: Should we be protecting our thyroids? Aust N Z J Surg 1999;69:847-8. [Google Scholar] |
| 10. | Herscovici D Jr., Sanders RW. The effects, risks, and guidelines for radiation use in orthopaedic surgery. Clin Orthop Relat Res 2000;375:126-32. [Google Scholar] |
| 11. | Verdun FR, Bochud F, Gundinchet F, Aroua A, Schnyder P, Meuli R. Quality initiatives* radiation risk: What you should know to tell your patient. Radiographics 2008;28:1807-16. [Google Scholar] |
| 12. | Giordano BD, Baumhauer JF, Morgan TL, Rechtine GR 2nd. Patient and surgeon radiation exposure: Comparison of standard and mini-C-arm fluoroscopy. J Bone Joint Surg Am 2009;91:297-304. [Google Scholar] |
| 13. | Burns S, Thornton R, Dauer LT, Quinn B, Miodownik D, Hak DJ. Leaded eyeglasses substantially reduce radiation exposure of the surgeon's eyes during acquisition of typical fluoroscopic views of the hip and pelvis. J Bone Joint Surg Am 2013;95:1307-11. [Google Scholar] |
Fulltext Views
4,134
PDF downloads
1,684




