Translate this page into:
Case of shoulder pain
Corresponding Author:
Nizar Abdulaziz Al-Nakshabandi
Department of Radiology, College of Medicine, King Saud University, Riyadh
Saudi Arabia
nizar97@hotmail.com
| How to cite this article: Al-Nakshabandi NA. Case of shoulder pain. J Musculoskelet Surg Res 2019;3:376-377 |
History
A 46-year-old Male complained of shoulder pain for more than 4 months. The pain was worse in the morning and relieved with activity. It was associated with stiffness in the neck and chronic low-back pain.
Physical Examination
Positive findings included limited chest expansion and severe loss of range of motion in the cervical and lumbar spine.
- hat are your findings?
- What is the differential diagnosis?
- What are the causes?
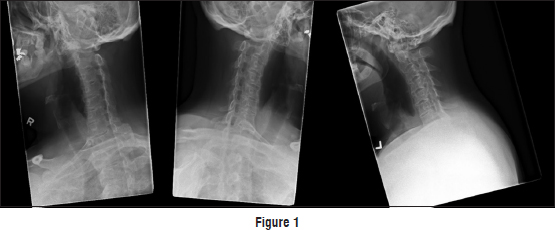
Findings
Vertebral alignment was maintained. Loss of lordosis of the cervical spine was likely related to ankylosis and spasm. There was evidence of vertebral body squaring with diffuse syndesmophytes, giving a bamboo spine appearance. Ankylosis of the apophyseal and costovertebral joints was seen. Narrowing of the intervertebral neural foramina was present from C2 to C7, being worse on the left side.
Differential Diagnosis
- General spine: Enteropathic arthritis
- Cervical spine: Juvenile rheumatoid arthritis
- Diffuse idiopathic skeletal hyperostosis.
Diagnosis
Ankylosing spondylitis.
Pearls and Discussion
Ankylosing spondylitis is a seronegative spondyloarthropathy, which results in the fusion of the spine (ankylosis) as well as ankylosis of the sacroiliac joint. It can also affect the large and small joints.
It affects males more commonly than females by a factor of 3:1. Male patients are usually affected in their 30s.
There is a 90% association with HLA-B27 gene. Rheumatoid factor is negative, hence the name seronegative spondyloarthropathy.
It can be associated with inflammatory bowel disease. Some patients with inflammatory bowel disease can have aortic valve disease/aortitis. In the eyes, it presents as uveitis and in the skin, it presents as psoriasis.
Sacroiliac joint is one of the first manifestations. The sacroiliac joint becomes widening before it narrows. In the end stage, the sacroiliac joint may not be seen.
In the spine, vertebral body squaring, a bamboo spine, interspinous calcification (dagger spine), shiny corners with erosions and sclerosis of the corners of the vertebral body are seen. The present case had a trapezial and costovertebral ankylosis.
Magnetic resonance imaging has a significant role in early diagnosis. Bone marrow edema of the sacroiliac joints is noted with synovial enhancement when gadolinium is administered.
The goal of treatment is to relieve pain and stiffness and prevent or delay complications and spinal deformity. Ankylosing spondylitis treatment is most successful before the disease causes irreversible damage to the joints. Physicians most commonly use nonsteroidal anti-inflammatory drugs (NSAIDs) to treat ankylosing spondylitis. They can relieve pain and stiffness. However, these medications might cause gastrointestinal bleeding.
If NSAIDs are not helpful, doctors suggest a biologic medication, such as a tumor necrosis factor (TNF) blocker or an interleukin 17 (IL-17) inhibitor.
TNF blockers help reduce pain, stiffness, and tender or swollen joints. They are administered by injecting the medication under the skin or through an intravenous line.
Secukinumab (Cosentyx®) is the first IL-17 inhibitor approved by the Food and Drug Administration for the treatment of ankylosing spondylitis.
TNF blockers and IL-17 inhibitors can reactivate latent tuberculosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Further Reading
- Riley MJ, Ansell BM, Bywaters EG. Radiological manifestations of ankylosing spondylitis according to age at onset. Ann Rheum Dis 1971;30:138 48.
- Resnick D, Niwayama G. Entheses and enthesopathy. Anatomical, pathological, and radiological correlation. Radiology 1983;146:1 9.
- Wilkinson M, Bywaters EG. Clinical features and course of ankylosing spondylitis; as seen in a follow up of 222 hospital referred cases. Ann Rheum Dis 1958;17:209 28.
Fulltext Views
1,997
PDF downloads
2,105




