
Translate this page into:
Combined intrafocal K-wire pinning for unstable pediatric distal forearm fractures
*Corresponding author: J. Terrence Jose Jerome, FRCS., EDHS. Department of Orthopaedics, Hand and Reconstructive Microsurgery, Olympia Hospital and Research Centre, Trichy, Tamil Nadu, India. terrencejose@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Jerome JTJ. Combined intrafocal K-wire pinning for unstable pediatric distal forearm fractures. J Musculoskelet Surg Res. doi: 10.25259/JMSR_405_2024
Abstract
This technical note presents a combined antegrade and retrograde intrafocal K-wire pinning technique for managing unstable and displaced distal third of the diaphysis fractures in older children (>10 years). While intrafocal pinning is established for distal radius fractures, its use in complex, unstable fractures in this age group is less explored. These fractures are prone to re-displacement, and single-direction pinning may be insufficient due to displacement severity, reduction challenges, or soft-tissue injury. The combined approach offers enhanced stability, particularly in older children at higher risk of re-displacement. The author reports good functional and radiological outcomes with no complications in their case series and details the surgical steps involved in this combined technique.
Keywords
Antegrade
Combined technique
Distal radius
Distal ulna
Fracture
Intrafocal
K-wire
Pinning
Retrograde
Unstable

INTRODUCTION
Distal forearm fractures are common in children, accounting for roughly one-third of all pediatric fractures, with a peak incidence around age 10.[1,2] While many of these fractures are incomplete (e.g., torus or buckle fractures) and heal well with simple immobilization, managing completely displaced fractures remains challenging. Closed reduction and casting often lead to high rates of redisplacement (7–91%), potentially causing malunion, functional limitations, and cosmetic concerns.[1,2] Studies have identified factors such as initial displacement severity, associated ulna fractures, and older age as predictors of poor outcomes with casting alone.[1,2] K-wire fixation has shown superior results compared to casting in displaced fractures,[3] but technical errors and neglecting ulna fracture fixation can still lead to complications.[2] A titanium elastic nailing system is another option, though optimal use and complication rates remain debated.[4-6] Plate fixation is reserved for complex cases (older age group, open fractures, severe comminution), and unstable displaced distal radius fractures due to the higher risk of complications.[5-8] There are unclear indications and a lack of consensus regarding treating unstable fractures in older children. These limitations in current treatment options for this age group highlight the need for a simple and practical approach.
Jerome has previously reported using antegrade intrafocal K-wire pinning for metaphyseal distal radius fractures in older children[9] and retrograde intrafocal K-wire pinning for physeal Salter-Harris II distal radius fractures.[10] While both techniques utilize intrafocal K-wire placement to achieve stability, they differ fundamentally in the direction of wire insertion relative to the growth plate. Antegrade pinning involves inserting the K-wires from the distal metaphysis toward the physis, while retrograde pinning involves inserting the K-wires through the physis and into the metaphysis. Despite this difference in approach, both techniques prioritize achieving stable fixation while minimizing damage to the growth plate. Building on these techniques, the author proposes a new surgical method combining antegrade and retrograde intrafocal K-wire pinning to treat displaced distal forearm both-bone fractures in older children. This combined approach aims to leverage the advantages of each technique to achieve optimal stability and minimize complications in this challenging fracture pattern. The purpose of this article is to describe this new, simple, and effective surgical method.
INDICATIONS
The combined antegrade and retrograde intrafocal K-wire pinning technique is particularly suitable for:
-
Unstable distal forearm fractures in older children (typically 10–16 years old), especially:
Completely displaced fractures with a high risk of redisplacement after closed reduction
Fractures remain unstable after reduction, necessitating surgical stabilization
Older children with limited remodeling potential, where anatomical reduction is critical.
CONTRAINDICATIONS
This technique is not recommended for:
Open fractures with severe contamination require more extensive surgical debridement and potentially different fixation methods
Severely comminuted fractures necessitating more rigid fixation, such as plate and screw constructs
Fractures with extensive articular involvement (e.g., Salter-Harris III and IV) that demand precise anatomical reduction and stable internal fixation to prevent long-term joint and physeal complications
Unreducible fractures or fragments where adequate alignment cannot be achieved, making K-wire fixation ineffective.
SURGICAL ANATOMY AND CONSIDERATIONS FOR DISTAL FOREARM FRACTURES IN CHILDREN
Understanding the pediatric forearm’s unique anatomy and growth patterns is crucial for successfully managing distal forearm fractures.
Key anatomical points
Radius and ulna relationship: The radius’s curved shape and rotation around the ulna during forearm movement are key considerations in fracture reduction and fixation.
Growth plates: The distal physis contributes significantly to forearm growth (75% for radius, 80% for ulna). This explains the higher remodeling potential of distal fractures compared to those near the elbow and also highlights the importance of protecting the growth plates during treatment.
Incomplete fractures, such as torus or buckle fractures, are common and generally stable. These cases typically require pain management and symptomatic care rather than extensive intervention.
Greenstick fractures involve angular deformity with an intact periosteal hinge. They are unstable and require close follow-up to prevent worsening angulation.
Complete fractures result in displacement and often shortening or angulation, demanding careful reduction and stabilization to avoid long-term complications.
Physeal Involvement: While the distal radius physis is frequently injured, the distal ulnar physis is less commonly affected. Physeal fractures necessitate meticulous management to prevent growth disturbances.
SURGICAL CONSIDERATIONS
Reduction and Stability: Achieving and maintaining proper alignment and stability are critical for optimal healing and function
Growth Plate Preservation: Any surgical intervention should minimize damage to the growth plates
Soft-tissue Considerations: Careful handling of surrounding soft tissues is essential to avoid complications such as nerve or tendon injury.
Understanding these anatomical and growth-related factors is fundamental for selecting the most appropriate treatment approach and optimizing outcomes in pediatric distal forearm fractures.
TREATMENT GOALS
The primary objective in treating pediatric forearm fractures is to ensure proper length, alignment, and rotation, facilitating normal function post-remodeling and healing. Normal forearm function involves an arc of motion for supination and pronation, totaling approximately 100°, evenly divided between the two movements. Given the remodeling capabilities in children, closed reduction and casting are commonly effective in achieving this. However, the reduction should fall within specific parameters to ensure optimal healing and function.
Most experts agree with the criteria established by Noonan and Price,[11] which outline acceptable reduction parameters that differ between younger patients (girls ≤8 years and boys ≤10 years) and older patients (girls >8 years and boys >10 years) [Table 1]. These guidelines have been debated in older children, with some advocating for more aggressive treatment approaches. For patients nearing skeletal maturity, anatomic reduction and potential surgical intervention are often preferred.
| Patient age | Distal shaft angulation | Midshaft angulation | Proximal shaft angulation | Rotation | Bayonet apposition |
|---|---|---|---|---|---|
| Girls≤8 years/Boys≤10 years | 15° | 15° | 15° | 15° | Up to 1 cm |
| Girls>8 years/Boys>10 years | 15° | 10° | 10° | 30° | Up to 1 cm |
ANESTHESIA AND PATIENT POSITIONING
The procedure is carried out under a supraclavicular block to provide regional anesthesia. The patient is positioned supine on the operating table, and an image intensifier is utilized to guide the placement of the K-wires and ensure accurate fracture reduction.
SURGICAL STEPS
Initial K-wire placement and fracture assessment
Three 1.8 mm K-wires are used for each case [Video 1]. A dorsal K-wire is first positioned using image intensifier guidance to align with the radius fracture site. A small dorsal skin incision is made, followed by careful soft-tissue dissection to create a pathway for the K-wire. This wire is then advanced through the fracture site, serving as a lever to help determine the appropriate reduction method.
Reduction techniques
Retrograde K-wire technique
This technique is preferred for dorsally displaced both-bone forearm fractures [Figure 1]. The K-wire is passed in a distal to the proximal direction (retrograde) through the fracture, leveraging the posterior cortex of the proximal radius fracture fragment. Once the reduction is deemed satisfactory, the K-wire is then drilled to pierce just the posterior cortex of the proximal radius, securing the alignment.

- Pre-operative radiographs demonstrating a displaced distal third of the diaphysis fracture in an 11-year-old boy.
Antegrade K-wire technique
The antegrade technique is employed when the retrograde method results in increased deformity or displacement instead of reducing the fracture. In this approach, the K-wire is passed from a proximal to distal direction (antegrade), leveraging the posterior cortex of the distal radius fracture fragment. Once a satisfactory reduction is achieved, the K-wire is drilled to pierce just the posterior cortex of the distal radius, ensuring stability.
Combined antegrade and retrograde technique for distal end radius fractures
In cases where the fracture is unstable or cannot be reduced using a single technique, a combination of both antegrade and retrograde K-wire pinning is employed. For instance, a dorsally displaced radius fracture typically requires a retrograde K-wire. However, if the retrograde technique worsens the deformity or makes reduction difficult, in that case, it indicates that the fracture is highly unstable, often due to significant periosteal and soft-tissue injuries that normally assist in fracture reduction [Figures 2 and 3]. In such situations, the surgeon should first use the antegrade K-wire to achieve the initial reduction [Figures 4-6], followed by the retrograde K-wires to secure stable fixation. This approach is also applicable in cases of volar displaced distal radius fractures. This combined method is especially effective for managing completely displaced and unstable both-bone fractures. All K-wires are inserted dorsally to avoid the volar side, thereby minimizing the risk of neurovascular and tendon injuries.
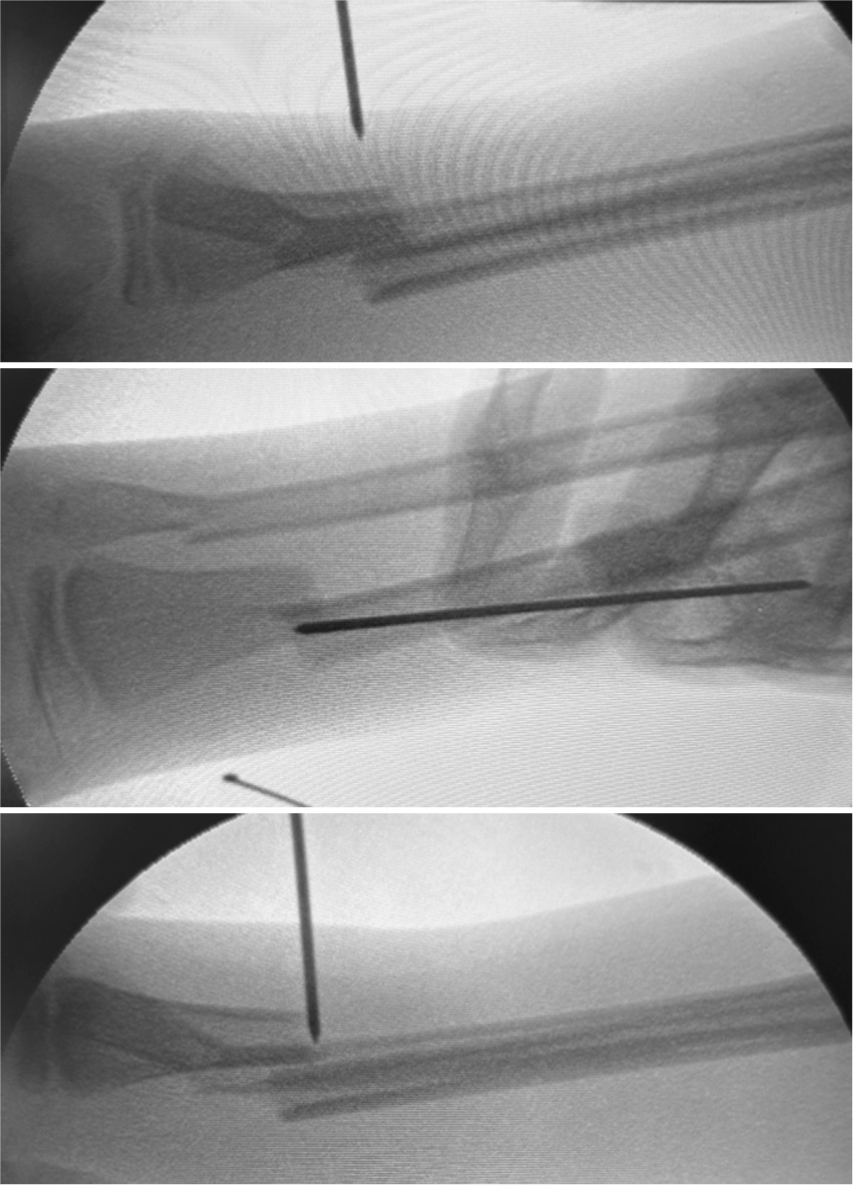
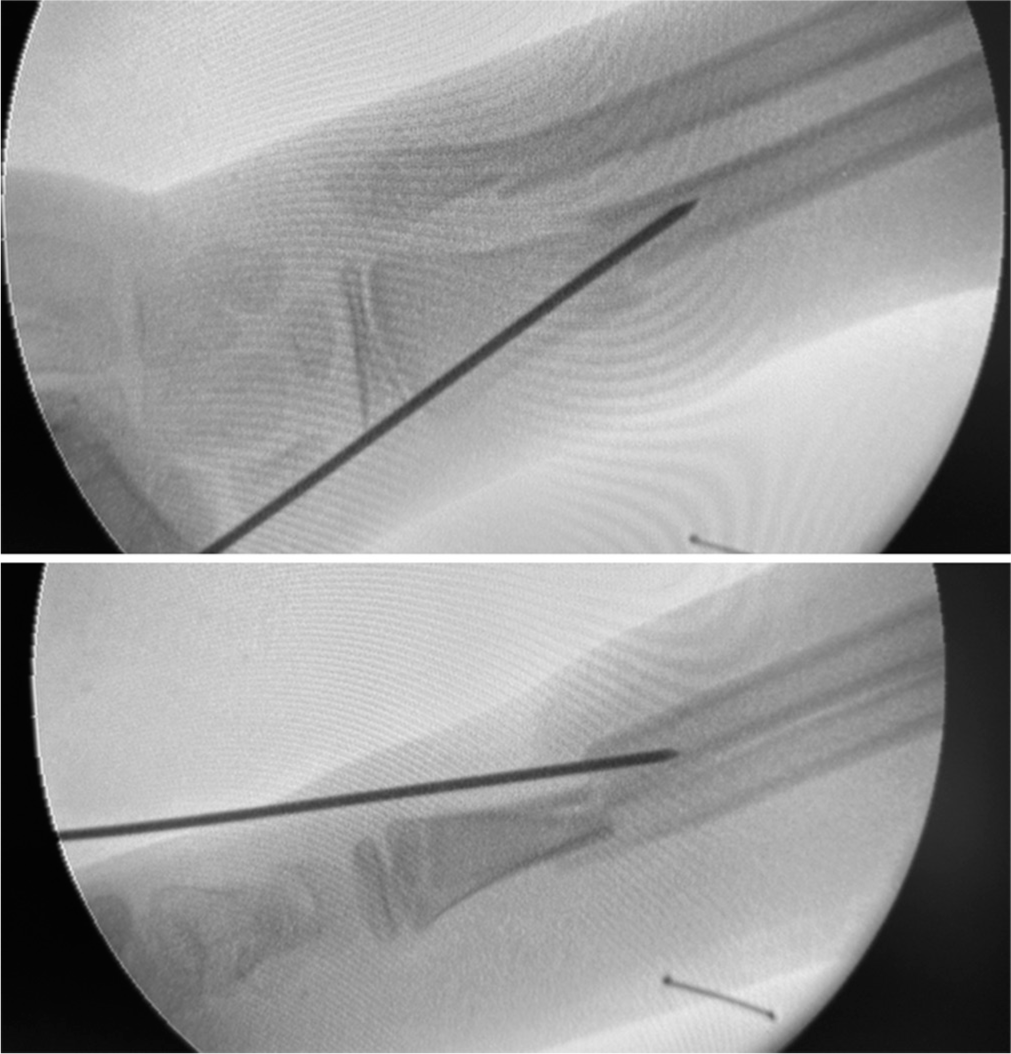
- Intraoperative fluoroscopic images showcasing the sequential steps of dorsal percutaneous K-wire insertion.

- An intraoperative fluoroscopic image illustrating how retrograde intrafocal K-wire insertion can exacerbate deformity and displacement in unstable radius fractures.
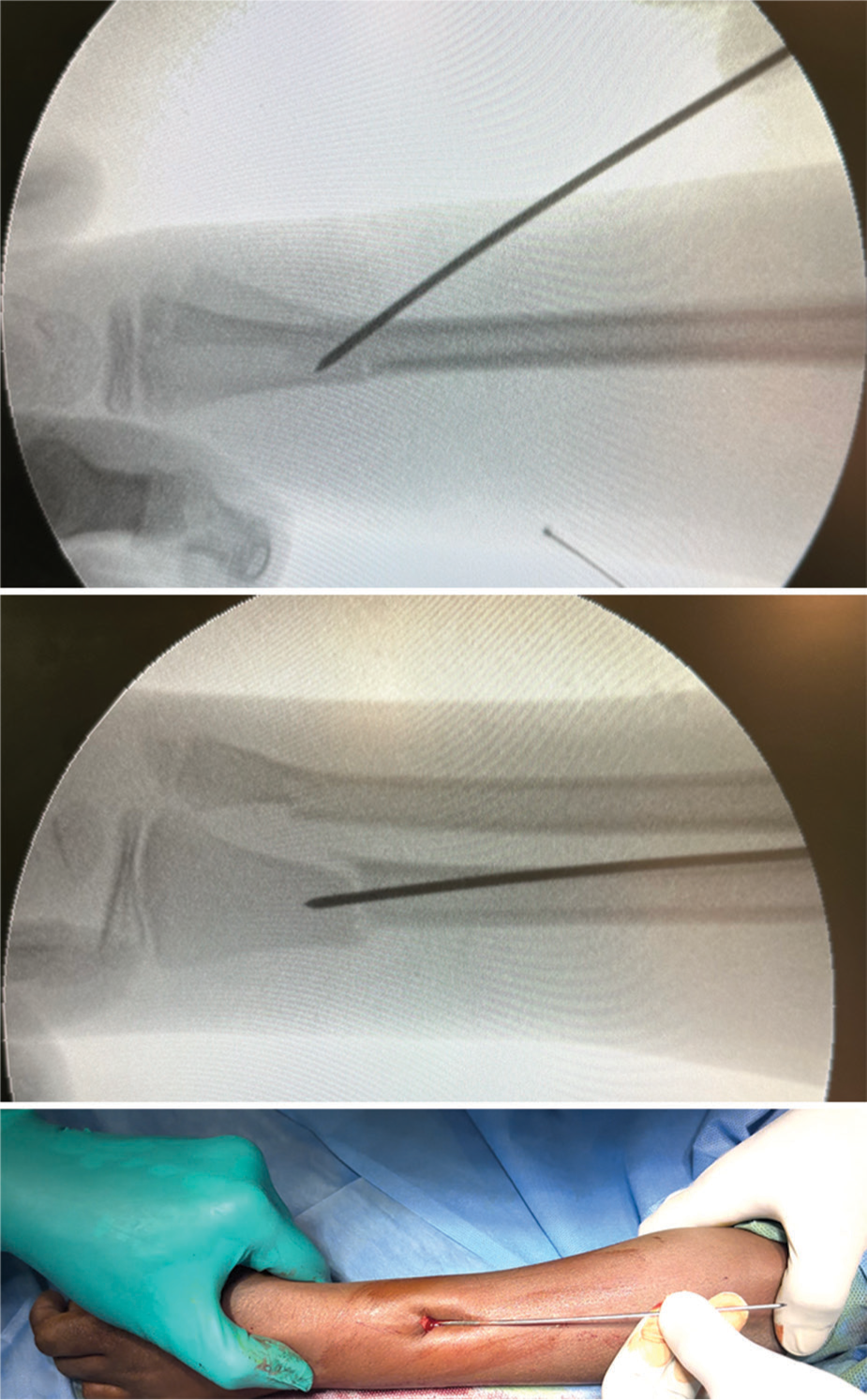
- An intraoperative fluoroscopic image demonstrating initial radius fracture reduction using the first antegrade K-wire.
- An intraoperative fluoroscopic image showing further reduction and stabilization of the radius fracture achieved with the second retrograde K-wire.
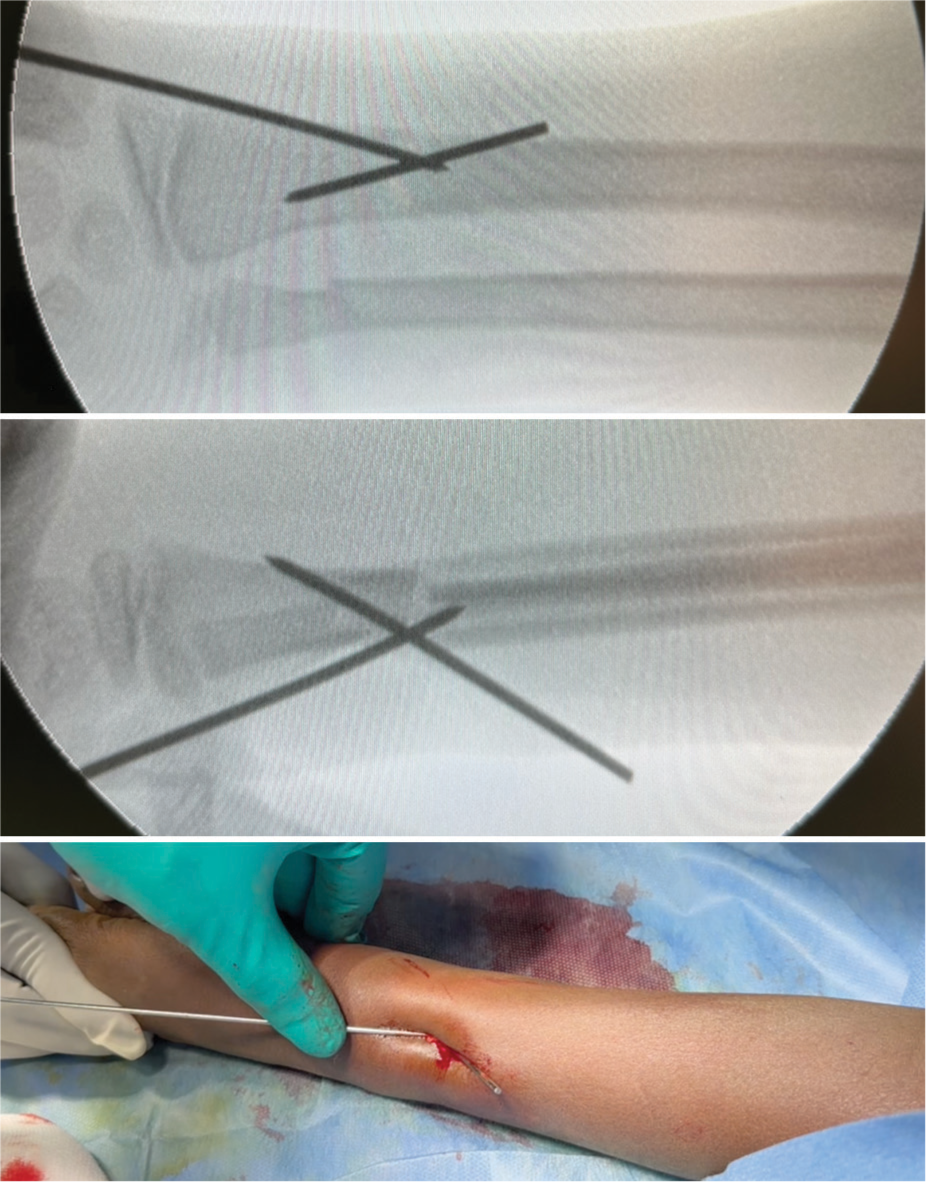
- An intraoperative fluoroscopic image highlights the final alignment and stabilization of the radius fracture fragments using the third antegrade K-wire.
Final radius fracture fixation
Three dorsal K-wires are utilized to achieve stable fixation of the fracture [Figure 7]. These wires are cut short and buried under the skin to reduce irritation and minimize the risk of infection. The small dorsal skin incisions made for wire placement may or may not require suturing, depending on their size and the surgeon’s discretion.

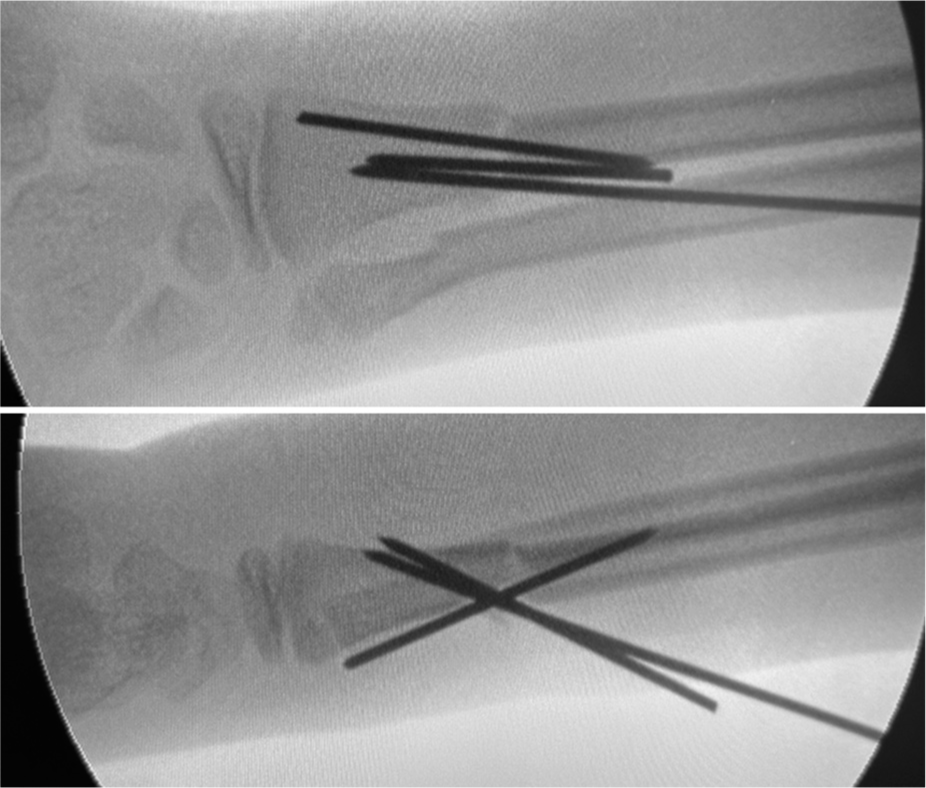
- An intraoperative fluoroscopic image depicting reduction of the distal ulna fracture with a retrograde K-wire.
Distal ulna fracture fixation
In most cases, stabilizing a distal radius fracture leads to indirect reduction of an associated distal ulna fracture. However, there are instances where the ulna remains displaced and unreduced, along with a displaced distal radioulnar joint (DRUJ). In such cases, the author recommends using the intrafocal K-wire pinning technique. This can be done using either the antegrade or retrograde technique, depending on the specific displacement of the fracture, to achieve proper alignment and stabilization of the ulna [Figure 8].
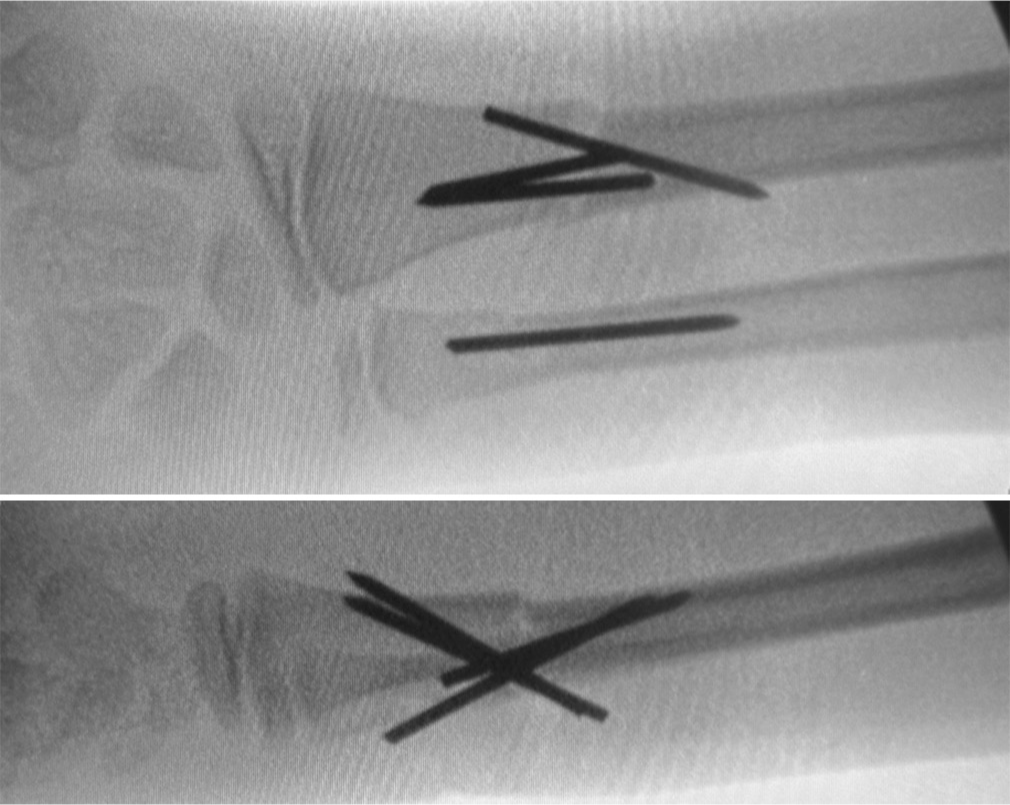
- Final intraoperative fluoroscopic image showcasing the successful reduction of both distal third of the diaphysis fractures using the combined antegrade and retrograde intrafocal K-wire pinning technique.
POST-OPERATIVE CARE
The patient is initially immobilized in an above-elbow splint for 3 weeks, followed by a below-elbow splint for another 3 weeks to support healing. After confirming radiological signs of union, the K-wires are removed at 6 weeks using local anesthesia in an office setting. Following removing the K-wires, the patient is allowed to resume normal activities immediately. Sports activities are encouraged after a period of 6–9 months to ensure full recovery and optimal function of the forearm.
ILLUSTRATIVE CASE
An 11-year-old boy fell at school, resulting in fractures of the right distal forearm. He presented with pain, swelling, and a noticeable deformity. Initial radiographs revealed dorsally displaced fractures of both the radius and ulna at the distal end. Due to the complete displacement of the fractures, an attempt at closed reduction was made under supraclavicular anesthesia. However, both fractures were not reducible, indicating severe periosteal and soft-tissue injury. Given the dorsal displacement and the author’s experience with intrafocal techniques, intrafocal K-wire pinning was planned. A dorsal K-wire was initially passed through the fracture using a retrograde technique to lever the fracture. However, this maneuver caused the dorsally displaced fracture to become volar displaced, indicating a highly unstable fracture with poor periosteal and soft-tissue support [Figure 9].
- An intraoperative fluoroscopic image illustrating how retrograde K-wire insertion can convert dorsal displacement to volar displacement in unstable, completely displaced fractures due to periosteal and soft-tissue injury.
Consequently, an antegrade technique was employed, passing the K-wire from proximal to distal. This effectively levered the posterior cortex of the distal radius and reduced the fracture. The K-wire was drilled through the posterior cortex and cut short. Another K-wire was introduced using the same wound in an antegrade manner, further stabilizing the fracture. Once satisfactory reduction was achieved, a third K-wire was placed using the retrograde technique to stabilize the proximal radius fracture from distal to proximal direction, ensuring stability and rotation control. Despite reducing the distal radius, the distal ulna remained displaced with a widened DRUJ, suggesting the fracture’s unstable nature and propensity for redisplacement if managed conservatively. Therefore, a dorsal intrafocal K-wire was passed through the ulnar fracture to achieve satisfactory reduction [Figure 10]. The patient was immobilized with an above-elbow splint for 3 weeks, followed by a below-elbow splint for an additional 3 weeks. K-wires were removed 6 weeks after confirming the radiological union. At the one-year follow-up, the patient demonstrated good functional and radiological outcomes [Figure 11].

- Three-week post-operative radiographs demonstrating acceptable fracture alignment in the illustrative case.

- One-year follow-up radiographs showing well-united distal third of the diaphysis fractures.
The author applied this technique to five older children with both-bone distal forearm fractures, with an average age of 12.5 years. The patients demonstrated an average pronationsupination arc of 140° and achieved a full range of motion in both the elbow and wrist. In addition, all patients reported a Visual Analog Score of 0, indicating no pain. There were no complications, and all patients achieved excellent radiological and functional outcomes at an average follow-up of 9 months.
COMPLICATIONS
Although the author has not encountered complications with this technique, it is important to recognize its potential risks. Superficial pin site infections, hypertrophic scars, neurapraxia, and hypertrophic granulation tissue are common complications associated with conventional K-wire pinning techniques. However, the author has successfully utilized intrafocal K-wire pinning with the wires cut short and buried beneath the skin, effectively minimizing these pin site complications. This technique not only reduces the risk of infection and other local issues but also prevents complications such as pin loosening, which can compromise fracture stability.
PEARLS
This combined antegrade and retrograde intrafocal K-wire pinning technique addresses a critical gap in managing unstable distal third of the diaphysis fractures in older children, a group with limited treatment options in the current literature. By offering enhanced stability, this approach proves to be more effective than single-direction pinning, especially for fractures with severe displacement, challenging reduction, or significant soft-tissue injury. It is particularly beneficial for older children over 10, who face a higher risk of redisplacement due to their active lifestyle and growth patterns. Utilizing dorsal K-wire insertion minimizes the risk of neurovascular and tendon injuries, contributing to a safer surgical approach. The case series and the author’s experience with this method indicate promising outcomes, with patients achieving good functional and radiological results without complications. In addition, the technique’s versatility allows it to be adapted to various fracture patterns and displacement types, facilitating personalized treatment for optimal patient outcomes.
PITFALLS
The combined antegrade and retrograde intrafocal K-wire pinning technique is technically demanding, requiring more surgical expertise than single-direction pinning. While the author reported no complications, the literature notes potential risks, including K-wire prominence, skin necrosis, redisplacement, neurapraxia, and scarring. In addition, there is a need for further evaluation of the long-term effects on growth and function, necessitating larger studies with extended follow-up periods. Careful patient selection is essential, as this technique may not be appropriate for all fracture types or younger children with different remodeling capabilities. There is also a learning curve associated with mastering this combined approach, which may pose a challenge for surgeons unfamiliar with its intricacies.
DISCUSSION
This technical note introduces a novel technique for stabilizing unstable distal third diaphyseal forearm fractures in older children: Combined antegrade and retrograde intrafocal K-wire pinning. This approach enhances stability, particularly in complex fractures with reduced remodeling potential, by utilizing dual-directional wire insertion. Promising outcomes observed in a case series highlight the potential for achieving functional and radiological success. While building on Kapandji pinning principles, our technique offers a novel solution for diaphyseal fractures in older children, addressing the specific biomechanical challenges and growth considerations in this population. Further investigation through larger, controlled trials with long-term follow-up is warranted to establish the efficacy and safety of this potentially valuable addition to the surgical armamentarium.
CONCLUSION
This technical note introduces a combined antegrade and retrograde intrafocal K-wire pinning technique for addressing unstable distal third of the diaphysis fractures in older children. This approach offers enhanced stability compared to single-direction pinning, particularly in this age group with high redisplacement risk. Early clinical experience suggests good functional and radiological outcomes without complications. While further studies are needed to establish its efficacy and safety definitively, this combined technique holds promise as a valuable tool for managing these challenging fractures, potentially offering a less invasive alternative to plate fixation with improved stability compared to traditional K-wire techniques.
ETHICAL APPROVAL
Ethical approval was obtained from the Ethical Committee Board, reference number OHRC/40/2024, dated September 3rd, 2024.
DECLARATION OF PATIENT CONSENT
The author certifies that he has obtained all appropriate patient consent forms. In the form, the patient’s parents have given their consent for the patient’s images and other clinical information to be reported in the journal. The parents understand that the patient’s name and initials will not be published, and due efforts will be made to conceal his/her identity, but anonymity cannot be guaranteed.
USE OF ARTIFICIAL INTELLIGENCE (AI)-ASSISTED TECHNOLOGY FOR MANUSCRIPT PREPARATION
The author confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Displaced fracture of the distal radius in children: Factors responsible for redisplacement after closed reduction. J Bone Joint Surg Br. 2005;87:841-3.
- [CrossRef] [PubMed] [Google Scholar]
- Re-displacement of stable distal both-bone forearm fractures in children: A randomised controlled multicentre trial. Injury. 2013;44:498-503.
- [CrossRef] [PubMed] [Google Scholar]
- Management of completely displaced metaphyseal fractures of the distal radius in children. A prospective, randomised controlled trial. J Bone Joint Surg Br. 2002;84:413-7.
- [CrossRef] [PubMed] [Google Scholar]
- Titanium elastic nailing radius and ulna fractures in adolescents. J Pediatr Orthop B. 2012;21:482-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric and adolescent forearm fractures: Current controversies and treatment recommendations. J Am Acad Orthop Surg. 2016;24:780-8.
- [CrossRef] [PubMed] [Google Scholar]
- Both bone forearm fractures in children and adolescents, which fixation strategy is superior-plates or nails? A systematic review and meta-analysis of observational studies. J Orthop Trauma. 2014;28:e8-14.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric diaphyseal forearm fractures: Epidemiology and treatment in an urban population during a 10-year period, with special attention to titanium elastic nailing and its complications. J Pediatr Orthop B. 2016;25:439-46.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical application of locked plating system in children. An orthopaedic view. Int Orthop. 2010;34:931-8.
- [CrossRef] [PubMed] [Google Scholar]
- Antegrade intrafocal Kapandji pinning technique for volar displaced distal radius fractures in older children. Eur J Plast Surg. 2024;47:57.
- [CrossRef] [Google Scholar]
- Salter-Harris II distal radial fractures treated with the intrafocal K-wire technique: A retrospective study of 20 cases. J Hand Surg Eur Vol. 2021;46:471-5.
- [CrossRef] [PubMed] [Google Scholar]
- Forearm and distal radius fractures in children. J Am Acad Orthop Surg. 1998;6:146-56.
- [CrossRef] [PubMed] [Google Scholar]




