
Translate this page into:
Dual sural flaps for bilateral foot degloving injuries: A case report
*Corresponding author: Thi Cao, Department of Orthopedics and Rehabilitation, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam. caothibacsi@ump.edu.vn
-
Received: ,
Accepted: ,
How to cite this article: Nguyen TN, Nguyen HM, Nguyen PD, Cao T. Dual sural flaps for bilateral foot degloving injuries: A case report. J Musculoskelet Surg Res. doi: 10.25259/JMSR_59_2025
Abstract
Bilateral degloving injuries of the feet are rare and challenging to reconstruct due to the extent of tissue loss and extensive exposed surface area. This case study describes the successful treatment of a 58-year-old male with bilateral foot degloving injuries using staged reconstruction with reverse sural artery flaps and split-thickness skin grafting. The surgical approach included vacuum-assisted closure therapy followed by large reverse sural artery flap harvests to restore plantar surfaces, complemented by split-thickness skin grafts for dorsal defects. Both flaps achieved full viability without complications, and the patient regained functional mobility after 12 months of rehabilitation. This report aimed to highlight the effectiveness of reverse sural artery flaps as a reliable alternative to free flaps in high-risk cases. It underscores the simplicity of this technique in achieving successful complex foot reconstruction while delivering favorable functional and esthetic outcomes.
Keywords
Degloving injuries
Foot reconstruction
Functional rehabilitation
High-energy trauma
Sural flap

INTRODUCTION
Degloving injuries of the foot are severe, high-energy traumas involving soft tissue avulsion and extensive exposure of underlying structures, including tendons, bones, and joints. Such injuries are rare, and the simultaneous occurrence of degloving injuries in both feet is exceedingly uncommon, posing substantial challenges for surgeons and patients striving to preserve the functional integrity of both limbs.[1,2]
Effective treatment requires meticulous reconstruction of the plantar soft tissues to withstand mechanical stress during recovery and ambulation while ensuring adequate coverage of dorsal skin defects to protect exposed tendons, bones, and joints from infection; prevent desiccation and necrosis; and promote optimal wound healing and functional recovery. While free flaps are frequently considered the gold standard for complex soft tissue reconstruction in modern microsurgery, their application in bilateral cases involving extensive defects is hindered by significant challenges, including an elevated risk of microvascular thrombosis due to vascular damage inherent to degloving injuries.[3-5]
Large reverse sural artery flaps offer a viable alternative, enabling the harvest of two independent flaps from each leg for complete plantar surface coverage. This relatively straightforward technique provides favorable esthetic results.[6] Despite an increased risk of venous congestion with large flaps, proper management ensures their effectiveness in addressing extensive bilateral degloving injuries. This report aimed to emphasize the utility of reverse sural artery flaps as a reliable and simple solution for complex foot reconstruction, achieving both functional and esthetic success in high-risk cases.
CASE REPORT
A 58-year-old male patient with no significant medical history arrived at our institution following a severe occupational accident. While operating industrial machinery, the patient slipped, resulting in both feet being entrapped in the machinery and sustaining complete degloving injuries [Figure 1]. Initial management, including first aid, pain control, and stabilization of vital signs, was undertaken at a local medical facility before referral to our tertiary care center, which specializes in orthopedic and reconstructive surgery and performs approximately 80 pedicle flap procedures monthly.
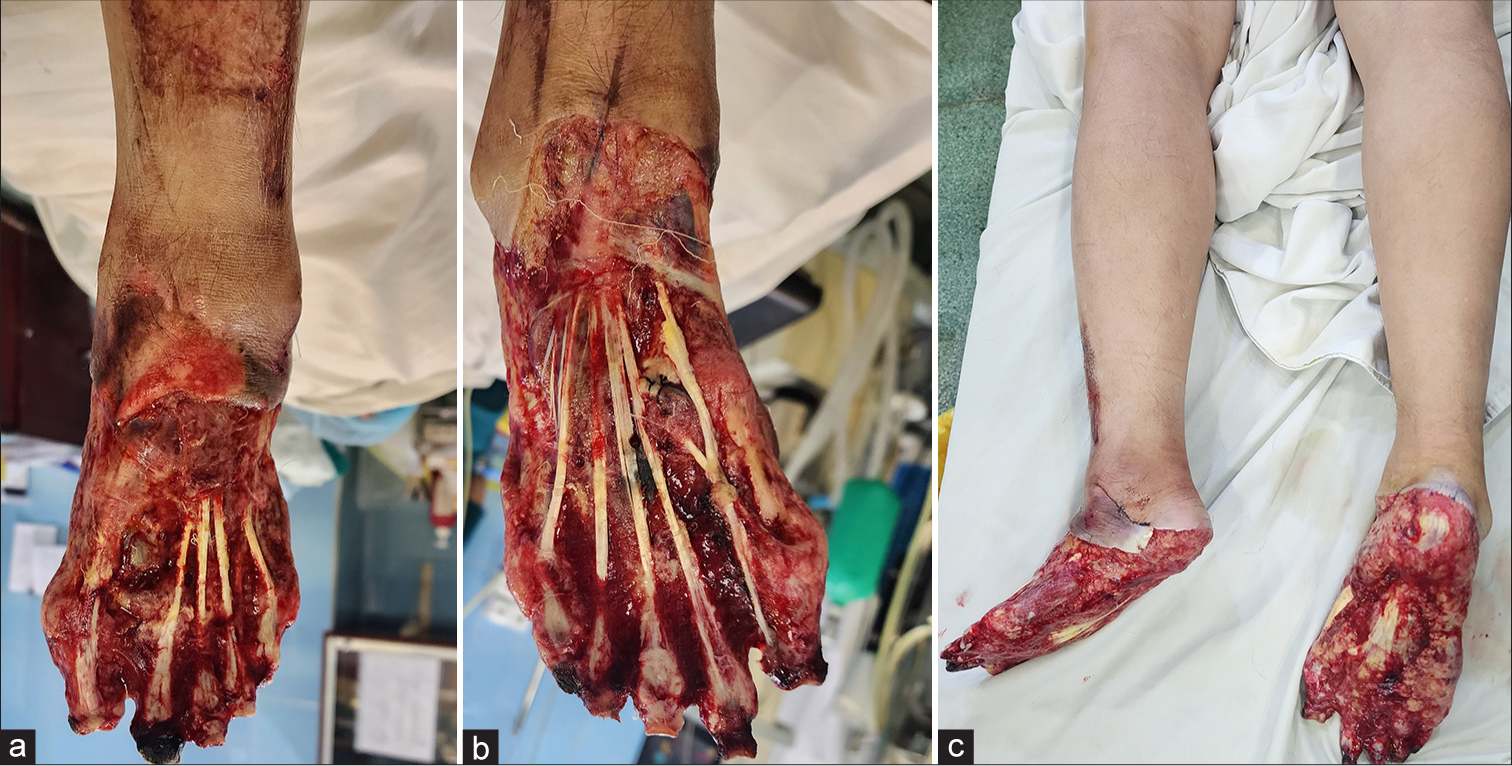
- Degloving injuries on both feet. (a and b) Dorsal view of the feet. (c) Plantar view of the feet.
Upon admission, the patient underwent emergency surgical debridement to remove devitalized tissue and was subsequently transferred to the plastic surgery department for definitive management of the bilateral foot injuries. Vacuum-assisted closure therapy was employed to stabilize the wound bed for 5 days. Subsequent assessment revealed extensive soft tissue damage, including total loss of the dorsal skin on both feet with exposure of extensor tendons and phalangeal bones, as well as complete loss of the plantar soft tissue padding bilaterally.
The surgical intervention was conducted in two stages:
Stage 1: Reconstruction of the left foot
Plantar surface: A large reverse sural artery flap was meticulously designed, with its distal point positioned at the popliteal fossa [Figure 2a]. The flap was elevated, incorporating a 3 cm wide adipofascial pedicle and a 1 cm wide strip of skin. A skin incision was made from the flap’s pivot point to the wound margin, followed by a “book-opening” dissection to accommodate the pedicle. The flap was then rotated to achieve full coverage of the plantar surface [Figure 2b]. The adipofascial pedicle was sutured into the prepared “book-opening” channel to ensure a flat and stable configuration, with the skin margins closed. The flap was secured loosely to the plantar surface to mitigate the risk of tension or vascular compromise.
Dorsal surface: The metatarsophalangeal joints were disarticulated, and the extensor tendons were excised completely. Split-thickness skin grafts harvested from the posterior aspect of the right thigh were applied to cover the dorsal surface of the foot [Figure 2c].
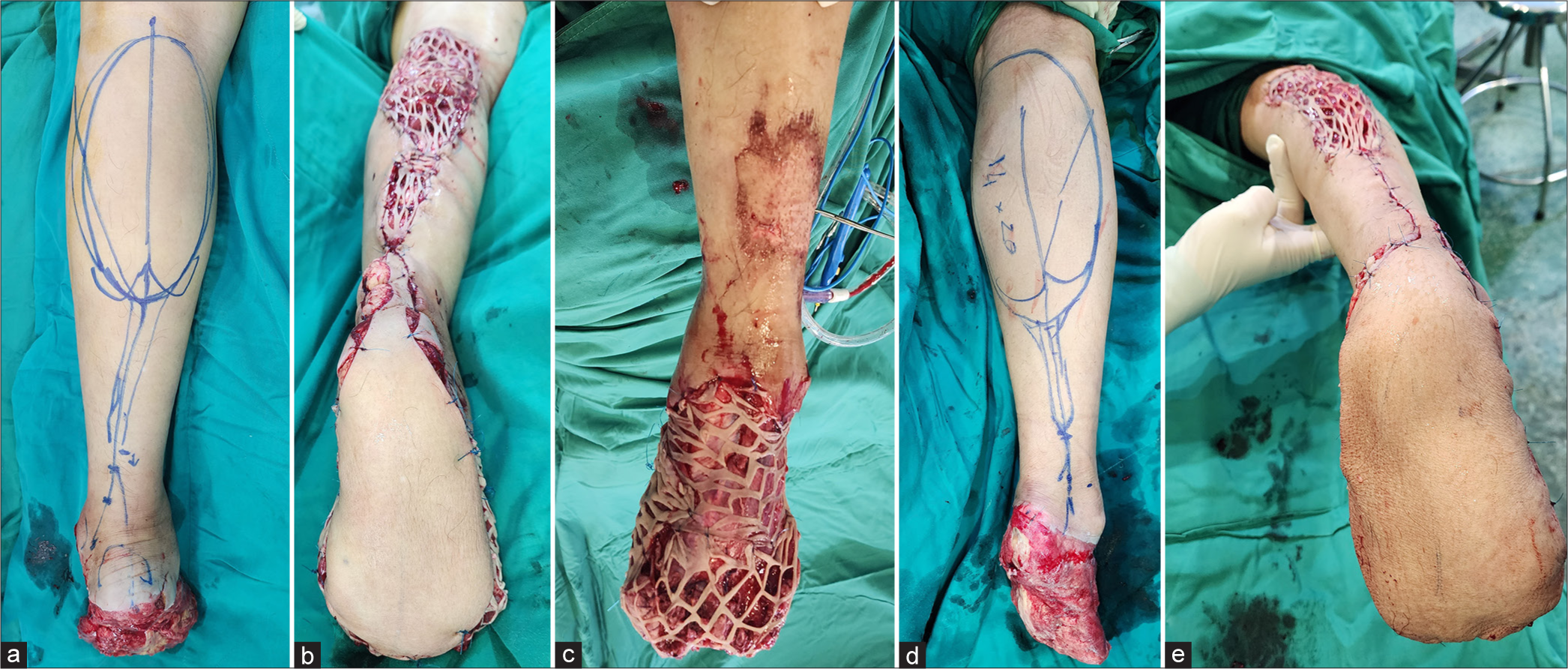
- Intraoperative images during soft tissue reconstruction for each foot. (a) Design of the sural flap for the left foot. (b) Rotation of the sural flap to cover the entire plantar surface of the left foot. (c) Thin skin graft on the dorsal and lateral surfaces of the left foot. (d) Design of the sural flap for the right foot. (e) Rotation of the sural flap to cover the plantar surface of the right foot.
Fourteen days postoperatively, the reverse sural artery flap exhibited full viability, with no evidence of venous congestion or other complications.
Stage 2: Reconstruction of the right foot
Fourteen days following the initial procedure, a similar surgical approach was implemented for the reconstruction of the right foot:
Dorsal surface: Split-thickness skin grafts were harvested and applied to cover the dorsal surface of the foot [Figure 2d].
Plantar surface: A large reverse sural artery flap, with its distal pivot point located at the popliteal fossa, was elevated and rotated to provide full coverage of the plantar surface of the right foot [Figure 2e].
Post-operative outcome
The sural flap on the right foot demonstrated full viability without any complications. Two weeks after the procedure’s completion, the patient was discharged in stable condition.
Follow-up and rehabilitation
The patient was enrolled in a structured follow-up and rehabilitation program, with scheduled evaluations every 2 weeks during the 1st month, monthly for the subsequent 6 months, and bi-monthly thereafter [Figure 3a and b].

- Post-operative images after sural flap rotation. (a) Post-operative view at 3 weeks. (b) Post-operative view at 6 weeks.
The rehabilitation protocol included the following:
Initial phase: Standing exercises were initiated with a support frame and footwear with soft insoles to minimize pressure on the reconstructed surfaces
Progressive weight-bearing: By the 3rd month, the patient could stand independently for approximately 10 min per session, with gradual increases in duration over time [Figure 4a and b]
Ambulation: By the 6th month, the patient commenced walking on the reconstructed plantar surfaces, demonstrating steady improvement in mobility and endurance
Long-term outcome: At the 12-month follow-up, the patient could walk comfortably without significant complications, achieving satisfactory functional recovery [Figure 5a and b].

- Follow-up at 4 months. (a) Images of the lateral and posterior aspects of the lower legs. (b) Plantar view of both feet.

- Follow-up at 12 months. (a) Plantar view of both feet. (b) The patient walks during daily life activities.
DISCUSSION
Degloving injuries are classified as severe due to their extensive soft tissue damage. When these injuries involve the feet, they not only cause significant soft tissue loss but also critically compromise the load-bearing function necessary for supporting body weight. Patients with complete degloving injuries of the feet are at high risk of permanent disability, often losing the ability to ambulate independently. In this case, bilateral degloving injuries posed a significant challenge in meeting the patient’s and family’s expectations of restoring mobility.[1]
Although modern microsurgical advancements prioritize free flaps for covering large defects, the specific risk factors associated with this patient’s injuries rendered free flaps an impractical choice. Degloving injuries frequently involve stretching and damage to the blood vessels at the interface of healthy and injured tissue, significantly increasing the risk of vascular thrombosis at microsurgical anastomoses.[7] Moreover, identifying a free flap sufficiently large to cover the entire plantar surface while maintaining an adequate vascular pedicle for ankle-level anastomosis posed substantial challenges, particularly when simultaneous reconstruction of both feet was required.[8]
The importance of a multidisciplinary approach and innovative solutions in managing complex trauma cases, such as crush and degloving injuries, has been well documented. Nguyen et al. (2024) highlight the critical role of surgical techniques, such as negative pressure wound therapy and meticulous reconstruction, in promoting wound healing and functional recovery following severe soft tissue trauma.[9] These findings further underscore the effectiveness of employing reverse sural artery flaps in this case, where a streamlined yet robust reconstruction method allowed for full coverage of extensive plantar defects, facilitating both functional and esthetic outcomes while minimizing complications.
In this context, the reverse sural artery flap emerged as an optimal alternative, offering several advantages, including the capacity to cover large defects, a straightforward surgical technique, and preservation of the primary vascular structures of the lower leg. Two large reverse sural artery flaps were sequentially utilized, providing complete coverage of the plantar surfaces for both feet. Venous congestion is one of the most common and concerning complications associated with this technique.[10] To minimize the risk of venous congestion, the flaps were loosely secured to the recipient sites, ensuring adequate space for expansion. Both flaps achieved full viability, resulting in favorable esthetic and functional outcomes. This approach successfully restored the patient’s ability to walk independently, meeting the expectations of both the patient and the medical team.
This clinical case highlights the efficacy of reverse sural artery flaps in managing complex degloving injuries while emphasizing the importance of tailoring reconstruction strategies to the specific characteristics of the injury and the patient’s condition. The success of this treatment not only reinforces the utility of reverse sural artery flaps but also illustrates the potential for innovative application of established surgical techniques in contemporary practice.
CONCLUSION
Bilateral degloving injuries of the feet pose a significant challenge in reconstructive surgery, even with modern advancements in microsurgical techniques. This case highlights the reverse sural artery flap as a reliable and effective reconstructive option, facilitating functional recovery, restoring mobility, and enhancing the patient’s quality of life. We consider the reverse sural artery flap a straightforward yet dependable solution for complex foot reconstruction, achieving both functional and esthetic success in high-risk cases.
Acknowledgment
The authors thank Tu Ngoc Nguyen, Ngan Ngoc Nguyen, and Duy Dinh Do for their help during the study.
Authors’ contributions
TNN and TC: Concepts, design, the definition of intellectual content, literature search, clinical studies, data acquisition, manuscript preparation, and manuscript editing. HMN: Clinical studies, data acquisition. PDN: manuscript preparation and manuscript editing. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
Ethical approval
The Institutional Review Board has waived the ethical approval for this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published, and due efforts will be made to conceal his/her identity, but anonymity cannot be guaranteed.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Conflicts of interest
There are no conflicting relationships or activities.
Financial support and sponsorship: This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Preserving the lower extremity after severe devolving injuries to meet the patient's demand in two cases: (Limb salvage after degloving injury) Trauma Case Rep. 2018;15:8-15.
- [CrossRef] [PubMed] [Google Scholar]
- Reconstruction of total degloving injuries of the foot in children. J Trauma Acute Care Surg. 2012;73:209-14.
- [CrossRef] [PubMed] [Google Scholar]
- Traumatic forefoot reconstructions with free perforator flaps. J Foot Ankle Surg. 2015;54:1025-30.
- [CrossRef] [PubMed] [Google Scholar]
- Management of foot degloving injury with bilateral anterolateral thigh flaps. Trauma Case Rep. 2023;45:100796.
- [Google Scholar]
- The free vastus lateralis muscle flap. A smart less used flap for soft tissue reconstruction of the weight-bearing foot. Injury. 2020;51:S34-40.
- [CrossRef] [PubMed] [Google Scholar]
- Utilizing a crossover reverse sural artery flap for soft tissue reconstruction of the plantar forefoot after a severe degloving injury. Int J Low Extrem Wounds. 2007;6:114-9.
- [CrossRef] [PubMed] [Google Scholar]
- The therapeutic challenges of degloving soft-tissue injuries. J Emerg Trauma Shock. 2014;7:228-32.
- [CrossRef] [PubMed] [Google Scholar]
- Lower extremity flap coverage following trauma. J Clin Orthop Trauma. 2019;10:839-44.
- [CrossRef] [PubMed] [Google Scholar]
- Comprehensive management of severe crush injury in a pediatric patient: A case report. Trauma Case Rep. 2024;54:101098.
- [CrossRef] [PubMed] [Google Scholar]
- The reverse sural artery flap-how do modifications boost its reliability? A systematic analysis of the literature. JPRAS Open. 2020;26:1-7.
- [CrossRef] [PubMed] [Google Scholar]




