
Translate this page into:
Effects of single-session high-intensity laser therapy on knee pain, joint position sense, and muscle strength in individuals with knee osteoarthritis: A pilot randomized controlled trial
 PhD, Tipwadee Bunprajun1PhD, Chutiporn Thammajaree1M ClinPhys, Nattapa Ariyakitsakul1MSc
PhD, Tipwadee Bunprajun1PhD, Chutiporn Thammajaree1M ClinPhys, Nattapa Ariyakitsakul1MSc
*Corresponding author: Prasert Sakulsriprasert, PhD. Faculty of Physical Therapy, Mahidol University, Salaya, Thailand. prasert.sak@mahidol.ac.th
-
Received: ,
Accepted: ,
How to cite this article: Tangsriwong K, Sakulsriprasert P, Bunprajun T, Thammajaree C, Ariyakitsakul N. Effects of single-session high-intensity laser therapy on knee pain, joint position sense, and muscle strength in individuals with knee osteoarthritis: A pilot randomized controlled trial. J Musculoskelet Surg Res. doi: 10.25259/JMSR_32_2025
Abstract
Objectives
Knee osteoarthritis (KOA) is a common musculoskeletal condition characterized by knee joint degeneration affecting intra-articular and surrounding structures. This causes pain and impaired knee joint position sense (JPS). This study aimed to investigate the effects of single-session high-intensity laser therapy (HILT) on knee pain, JPS, and muscle strength in individuals with KOA.
Methods
Ten females aged over 50 were recruited. Knee pain was measured with a Visual Analog Scale, and joint reposition error angle and muscle strength were obtained at baseline, immediately post-intervention, and 24 h post-intervention. The block randomization was done to an active HILT or a placebo HILT group.
Results
The between-group difference in knee pain, joint reposition error angle, and muscle strength was not found. However, knee pain was statistically significant at the immediate post and 24-h intervention in the active HILT group (P = 0.014). Normalized knee flexor and extensor muscle strength slightly increased immediately after post and 24-h intervention in the active HILT group.
Conclusion
This pilot study investigated the single-session intervention of HILT in individuals with KOA. The trend was found to alleviate pain and strengthen knee muscles.
Keywords
Hamstring
Joint position sense
Knee
Laser therapy
Osteoarthritis
Quadriceps
Rehabilitation

INTRODUCTION
Knee osteoarthritis (KOA) is evident with the knee joint degeneration involving all intra-articular and surrounding structures.[1,2] KOA impacts not only joint function, disability, and quality of life but also economic costs.[3] Pain is a common symptom in the KOA that occurs after microtrauma in daily activities, which induces chemical inflammation leading to joint capsule effusion. The synovial fluid increases pressure inside the knee joint and reduces mechanoreceptor sensitivity by pain-disrupting signals to the central nervous system.[4,5] Most individuals with KOA experience joint pain, swelling, stiffness, and limited movement, which affect joint position sense (JPS).[6,7] Impaired JPS had a relationship with the progression of the KOA stage, severity, and quality of life.[6] In addition, KOA reduces muscle strength from disuse or reflex inhibition caused by pain affecting muscle contraction force.[8] Therefore, effective treatment strategies are necessary due to impaired proprioception and muscle weakness.
High-intensity laser therapy (HILT) has a higher energy density to targeted structures, allowing deeper structures to absorb the photon rather than low-level laser therapy (LLLT).[9] A recent study reported that HILT was effective in pain reduction, function, range of motion, and quality of life improvement.[10] For KOA, several previous studies have reported that HILT effectively alleviates pain and improves function and structures.[11-15] However, the aforementioned studies have prescribed multiple sessions of HILT interventions. Practically, individuals with KOA have to comply with the suggested HILT regimen regarding multiple sessions per week and also the cost of treatment. It is interesting to investigate the effects of single-session HILT in individuals with KOA, such as the cost, practicality, or patient compliance considerations. This study, therefore, aimed to study the effectiveness of single-session HILT in managing knee pain, JPS, and muscle strength in individuals with KOA.
MATERIALS AND METHODS
Study design
The study was designed to be a pilot double-blind, randomized controlled trial. The data were collected at the Faculty of Physical Therapy (Physical Therapy Center), Mahidol University.
Participants
Ten female individuals with KOA aged 64.4 years were recruited into this study. The inclusion criteria were age over 50 years, knee pain greater than 3 on the Visual Analog Scale (VAS) during aggravation, the duration of knee pain lasted more than 3 months, diagnosed with unilateral KOA by a physician or meeting the American College of Rheumatology Classification Criteria for clinical KOA,[16] which includes knee pain and at least three additional criteria (no palpable warmth, presenting with stiffness less than 30 minutes, crepitus, bony enlargement, and bony tenderness). The severity of KOA was classified as grades 0–3 according to the Kellgren–Lawrence classification,[17] with no specific treatments, such as steroid injections, within the 3 months before this study. Exclusion criteria were any other musculoskeletal problems associated with knee pain such as tendon or ligament tear, meniscus injury, fracture, rheumatoid arthritis, knee surgery, or back pain, any musculoskeletal conditions at the hip and ankle joints, lower limb fracture, neurological conditions such as stroke or Parkinson’s disease, contraindications for laser therapy, such as a tumor, cancer, bleeding at the knee joint, abnormal sensation, or tattoo. We have not calculated the sample size since we initiated the pilot study. Therefore, we recruited 10 eligible subjects for analysis.
Randomization and blinding
The participants were randomly allocated into 2 groups (active HILT and placebo HILT) with block randomization technique using a web-based program, www.randomizer.org, through a block randomization technique with body mass index (BMI) and age as the criterion for randomization. The participants were blinded to group allocation and HILT application, while a measurement researcher was blinded to group allocation.
Outcome measures
Knee pain
The participants rated the pain on the worst movement, using a 10-cm VAS with “no pain” indicated at the left end and “the worst pain imaginable” at the right end. The researcher recorded the distance between the left endpoint and the participants’ mark and wrote it in the data collection form. A previous study reported the clinical significance of pain reduction from the minimal clinically important difference for VAS, which was 2.26 cm.[18]
Knee JPS
A joint position repositioning technique was used. The participants were measured with a smartphone application, “Measure App” (iPhone 12 Pro Max, Apple Inc., USA). The smartphone was attached to the shank of the tibia at the malleolar level. The participants sat in the starting position with knee flexion at 90°. Then, the participants with eyes closed were actively guided to the 45° knee flexion and held for 3 s. Then, participants relaxed their legs to the starting position, 90° knee flexion, and rested for 5 s. In the testing session, the participants reproduced the angle when they thought they would reach the targeted angle of 45° knee flexion and held their knees at that angle. The measurement researcher recorded the angle from the Measure App application. The absolute value obtained from the difference between the performed and targeted angles was recorded as the joint reposition error angle. The participants performed 3 times. The average value was used for the analysis.[19] Our test-retest reliability [intraclass correlation coefficient (ICC3,1)] for the JPS measurement was 0.749, the standard error of measurement was 1.27, and the minimal detectable change was 3.52.
Knee muscle strength
The muscle strength of both the knee flexor and knee extensor muscles was measured using a handheld dynamometer (Model 01165A, Lafayette Instrument, USA). An isometric “make” test was employed, following a pain-free approach throughout the assessment.
Participants were seated with their hips and knees flexed at 90° to measure knee flexor muscle strength. The dynamometer was positioned on the posterior aspect of the shank, just proximal to the ankle joint. The measurement researcher provided static resistance against the participants’ maximum isometric knee flexion force, which was recorded in kilograms. The participants were asked to complete two trials, with the highest value from these trials used for analysis. For the knee extensor muscle assessment, the testing procedure was the same as the knee flexor strength measurement, but the dynamometer was placed on the anterior aspect of the shank, proximal to the ankle joint.[20] The normalized value was used for statistical analysis by computing the normalized value = actual force (kilograms) divided by the participant’s body weight (kilograms). Our test-retest reliability (ICC3,1) for the knee flexor was = 0.931, and the knee extensor was 0.963.
Interventions
For the active HILT group, the pulsed ND: YAG high-intensity laser (HIRO 3, ASA Srl, Italy), a wavelength of 1064 nm, peak power of 3 kW, maximum average power of 10.5 W, energy density of 4 J/cm2, and a pulse duration < 100 µs, with a DJD handpiece [Figure 1], was used by the experienced physical therapist for a single session. The handpiece was positioned vertically in contact during laser beam delivery to the surface area. The participants were supine with 30° knee flexion for anterior aspect scanning and prone lying for posterior aspect scanning.
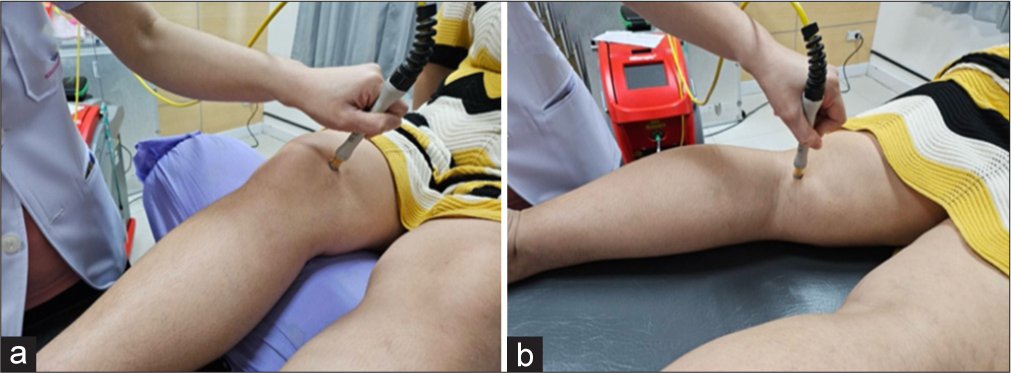
- Position of handpiece on irradiation points (a) Supine (b) Prone.
In this study, HILT intervention was done in 3 phases: (1) The initial phase, a fast manual scanning along the anterior, medial, and lateral aspects of the knee joint between femoral and tibial epicondyles in 300 cm2 approximately, with 2 subphases of 710 mJ/cm2 and 810 mJ/cm2, total energy of 500 J; (2) the intermediate phase, the handpiece was applied on the trigger or tender point of total 8 points at the medial and lateral epicondyle of tibia and femur, medial and lateral knee joint line, and tendon of biceps femoris and semitendinosus muscles[21] with 25 J, a fluency of 610 mJ/cm2, 14 s for each point, a total energy 250 J; and (3) the final phase, a slow manual scanning as initial phase, total energy of 500 J, 1,250 J in total per one session.
During the treatment, the participants wore safety goggles for eye protection. The participants who underwent the placebo HILT group received placebo HILT, which was the same treatment technique and position as active HILT, but the laser was not emitted.
Study procedure
The participants were allocated into two groups using a web-based program, www.randomizer.org, through a block randomization technique with BMI and age as the criterion for randomization. Randomization procedures blinded the participants and the measurement researcher. The same measurement researcher assessed all participants. The assessments were performed three times: baseline (T0), immediately post-intervention (T1), and 24 h post-intervention (T2). Ten women with KOA were eligible following the inclusion and exclusion criteria. Each group consisted of 5 participants who underwent active HILT or placebo HILT. The participants who underwent active HILT received HILT.
Meanwhile, the placebo HILT received sham HILT and then received active HILT after the study, after 24-h post-intervention measurements. Both groups received a pamphlet detailing pain education regarding self-care management for KOA. All patients were instructed to abstain from using pain medications; however, they were permitted to engage in their usual activities of daily living throughout the data collection period. The CONSORT diagram is shown in Figure 2.
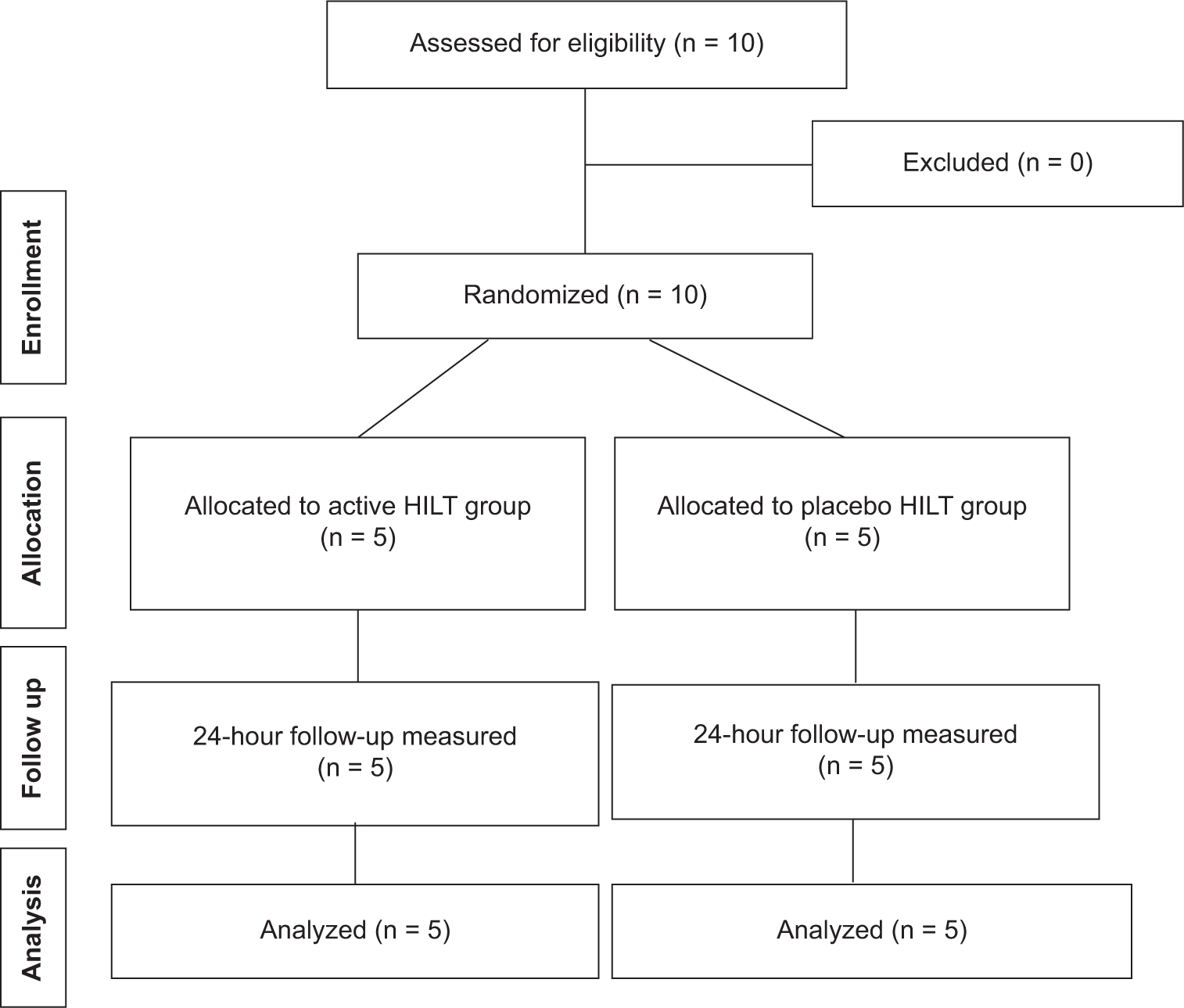
- CONSORT diagram of the study. HILT: High-intensity laser therapy.
Statistical analyses
The Statistical Package for the Social Sciences software version 23 (IBM, Armonk, NY) was used for data analyses. The data were presented in mean ± standard deviation. The data in this study were normally distributed and checked using the Shapiro–Wilk test. An independent samples t-test was used to compare demographic data between groups. A two-way mixed analysis of variance with repeated measures was used to analyze the main effects of time, group, and their interactions. If significant main effects were identified, Bonferroni post hoc analysis was conducted for multiple comparisons. The P < 0.05 was set as the statistical significance.
RESULTS
The demographic data of all participants regarding age, weight, height, body mass index, and duration of symptoms were not different between the two groups (P > 0.05) [Table 1]. There were no significant differences between the groups’ baseline values of VAS, JPS, quadriceps, and hamstring muscle strength.
| Active HILT (n=5) | Placebo HILT (n=5) | P-value | |
|---|---|---|---|
| Age (year) | 66.80±2.62 | 62.00±2.43 | 0.216 |
| Weight (kg) | 55.60±1.16 | 62.78±4.45 | 0.157 |
| Height (m) | 1.55±0.03 | 1.55±0.02 | 0.961 |
| BMI | 23.24±0.99 | 25.99±1.39 | 0.146 |
| Duration of symptom (months) | 27.40±15.40 | 25.60±7.96 | 0.220 |
Values are presented as mean±standard deviation, HILT: High-intensity laser therapy, BMI: Body mass index
For knee pain, there was a significant difference in time effect (F = 5.630, P = 0.014), the effect size was 4.13, no difference in group effect (F = 0.176, P = 0.686), and no difference in interaction (F = 2.287, P = 0.169) [Table 2]. However, post hoc analysis for the time effect did not detect significant differences in either group.
| Variables | Group | T0 | T1 | T2 | T0-T1 | T0-T2 | P-value |
|---|---|---|---|---|---|---|---|
| VAS pain (cm) | HILT Placebo |
6.20±0.40 4.76±0.63 |
3.54±1.11 3.06±0.95 |
2.96±1.17 3.70±0.90 |
2.66±2.35* 1.70±1.98 |
3.24±2.80* 1.06±1.59 |
0.014* |
| Joint position sense error (°) | HILT Placebo |
5.67±1.85 4.20±1.11 |
5.27±0.86 2.60±0.87 |
6.53±1.76 4.00±1.38 |
0.40±3.85 1.60±2.07 |
−0.87±7.13 0.20±2.93 |
0.572 |
| Normalized knee flexor muscle strength (kg/BW) | HILT Placebo |
0.08±0.02 0.11±0.03 |
0.09±0.03 0.13±0.02 |
0.12±0.01 0.13±0.02 |
0.00±0.03 −0.02±0.03 |
−0.03±0.03 −0.02±0.03 |
0.397 |
| Normalized knee extensor muscle strength (kg/BW) | HILT Placebo |
0.19±0.08 0.26±0.06 |
0.21±0.08 0.23±0.04 |
0.23±0.05 0.26±0.06 |
−0.02±0.05 0.03±0.05 |
−0.04±0.05 0.00±0.08 |
0.067 |
Values are presented as mean±standard deviation. VAS: Visual Analog Scale, BW: Body weight, HILT: High-intensity laser therapy, T0: Baseline assessment, T1: Immediately post-intervention, T2: 24-h post-intervention. *Denotes a significant difference
In the JPS error, there was a significant difference in the time effect (F = 0.579, P = 0.572), no difference in the group effect (F = 3.294, P = 0.107), and no difference in the interaction (F = 0.130, P = 0.879).
For normalized quadriceps muscle strength, there was a significant difference in time effect (F = 0.979, P = 0.397), no difference in group effect (F = 2.525, P = 0.151), and no difference in interaction (F = 1.035, P = 0.378). For normalized hamstring muscle strength, there was a significant difference in time effect (F = 3.208, P = 0.067), no difference in group effect (F = 4.020, P = 0.080), and no difference in interaction (F = 0.868, P = 0.439).
DISCUSSION
This study was initiated to investigate a single-session HILT intervention for individuals with KOA. We aimed to focus on the effects of HILT on pain intensity, JPS, and knee muscle strength immediately after the HILT intervention and within 24 h. All participants were female, which was beneficial in controlling the sex factor and presenting the majority because of its higher prevalence.[2]
The active HILT group showed a clinically significant reduction in pain that lasted 24 h after a single-session HILT compared to the placebo HILT. This study’s magnitudes of pain change, 2.66 cm immediately post and 3.24 cm at 24 h, were clinically meaningful since the minimal clinically important difference for VAS in knee arthroplasty patients was 2.26 cm.[18] Therefore, this finding affirmed the analgesic effects of HILT, which can be explained by several mechanisms, such as the gate control system,[11] ATP production, and reactive oxygen species modulation.[10,22] The results also provided valuable information for clinicians when making decisions regarding the frequency of HILT programs, suggesting that daily intervention may not be necessary. It also aids in the design of therapeutic exercise programs for patients with KOA during periods of pain reduction. However, future studies should explore additional outcomes related to functional status and quality of life, which would assist clinicians in adopting a more holistic approach and designing more effective therapeutic programs. In addition, no adverse effects were found in this study.
Previous studies showed that KOA patients had impaired knee joint position from various structures.[6,7] Our study found that the values of absolute errors were likely to decline immediately and increase after 24 h. Even though the pain in the active HILT group was significantly decreased, this could not sufficiently contribute to joint reposition error reduction. We, therefore, suggested increasing the intervention sessions and extending the study duration since the recovery of various structures responsible for knee JPS, both active and passive structures, might take more intervention sessions and a longer healing process.
Knee muscle strength plays a critical role in regulating knee joint position, as muscle weakness can impair proprioceptive accuracy.[23] This study assessed knee flexor and extensor muscle strength to examine the effects of HILT. Results showed a slight improvement in knee muscle strength in the active HILT group. However, this increase did not reach statistical significance. The insignificant results for both JPS and knee muscle strength might suggest that a single session of HILT was insufficient for improving both JPS and knee muscle strength. A previous study found that HILT plus exercise showed significantly increased knee muscle strength during the post-intervention at 3rd-week and 3rd-month follow-up compared to the placebo plus exercise.[24] However, how many sessions are necessary to improve JPS and knee muscle strength remains unclear. Future studies should monitor these variables over a longer duration and incorporate multiple assessment time points. In addition, this study did not use tele-rehabilitation but it was effective in managing KOA patients.[25] Therefore, future studies could incorporate telerehabilitation into the management plan for KOA patients.
Study limitations
There were several limitations in this study. Although there were no restrictions on sex during recruitment, all participants were female, as only female patients were available for inclusion. We recruited only 10 females with KOA. Although clinical significance was observed in pain reduction within the active HILT group, we recommend increasing the sample size to detect better significant changes in pain, JPS, and knee muscle strength. In addition, we recommend measuring other variables, such as range of motion, functional capacity, and quality of life, to better understand the clinical and overall perspectives of individuals with KOA. The patients in this study had no radiological grading for osteoarthritis, information about sociodemographic data, comorbidities, employment status, and patient physical activity. Finally, the study duration was restricted to a maximum of 24 h, which constrained the ability to assess longer-term effects and limited the number of time points for data collection.
CONCLUSION
This study was a pilot study to investigate the single-session intervention of HILT in individuals with KOA. The results were detected toward pain reduction and knee muscle strength promotion after a single-session intervention of HILT.
Recommendations
Single-session intervention of HILT was promising in pain reduction for individuals with KOA since pain could inhibit exercise and activities of daily living. Therefore, clinicians can select HILT as an intervention for pain alleviation.
Authors’ contributions
PS, KT, and TB: Conceived and designed the study, conducted research, and provided research materials. KT, CT, and NA: Collected and organized the data. PS and KT: Analyzed and interpreted data and wrote the initial and final drafts of the article. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
Ethical approval
This study was approved ethically by the Mahidol University Central Institutional Review Board (MUCIRB) following the Declaration of Helsinki, COA no. MU-CIRB 2024/003.0401, dated 4 January 2024, and registered clinical trial from ClinicalTrials.gov, Identifier: NCT06632119.
Declaration of participant consent
The authors certify that they have obtained all appropriate participant consent forms. In the form, the participants have given their consent for their images and other clinical information to be reported in the journal. The participants understand that their names and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Conflicts of interest
There are no conflicting relationships or activities.
Financial support and sponsorship: This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Factors associated with functional impairment in symptomatic knee osteoarthritis. Rheumatology (Oxford). 2000;39:490-6.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology and burden of osteoarthritis. Br Med Bull. 2013;105:185-99.
- [CrossRef] [PubMed] [Google Scholar]
- Economic and humanistic burden of osteoarthritis: A systematic review of large sample studies. Pharmacoeconomics. 2016;34:1087-100.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of joint effusion on proprioception in patients with knee osteoarthritis: A single-blind, randomized controlled clinical trial. Osteoarthritis Cartilage. 2011;19:22-8.
- [CrossRef] [PubMed] [Google Scholar]
- Can pain influence the proprioception and the motor behavior in subjects with mild and moderate knee osteoarthritis? BMC Musculoskelet Disord. 2014;15:321.
- [CrossRef] [PubMed] [Google Scholar]
- Proprioception in knee osteoarthritis: A narrative review. Osteoarthritis Cartilage. 2011;19:381-8.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation among proprioception, muscle strength, and balance. J Phys Ther Sci. 2016;28:3468-72.
- [CrossRef] [PubMed] [Google Scholar]
- Quadriceps arthrogenic muscle inhibition: the effects of experimental knee joint effusion on motor cortex excitability. Arthritis Res Ther. 2014;16:502.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of high-intensity laser therapy in the treatment of musculoskeletal disorders: A systematic review and meta-analysis of randomized controlled trials. Medicine. 2018;97:e13126.
- [CrossRef] [PubMed] [Google Scholar]
- High-intensity laser therapy for musculoskeletal disorders: A systematic review and meta-analysis of randomized clinical trials. J Clin Med. 2023;12:1479.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of high intensity laser therapy for reduction of pain in knee osteoarthritis. Pain Res Manag. 2016;2016:9163618.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of high intensity laser therapy in knee osteoarthritis: A double-blind controlled randomized study. Clin Rheumatol. 2021;40:1989-95.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of pulsed Nd: YAG laser in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers Med Sci. 2017;32:503-11.
- [CrossRef] [PubMed] [Google Scholar]
- A randomized comparative study between high-intensity laser vs low-intensity pulsed ultrasound both combined with exercises for the treatment of knee osteoarthritis. Int J Rheum Dis. 2022;25:877-86.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of high-intensity laser therapy in the management of patients with knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. J Back Musculoskelet Rehabil. 2020;33:875-84.
- [CrossRef] [PubMed] [Google Scholar]
- Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986;29:1039-49.
- [CrossRef] [PubMed] [Google Scholar]
- Radiological assessment of osteoarthrosis. Ann Rheum Dis. 1957;16:494-502.
- [CrossRef] [PubMed] [Google Scholar]
- How much pain is significant? Defining the minimal clinically important difference for the visual analog scale for pain after total joint arthroplasty. J Arthroplasty. 2018;33(7S):S71-5.e2.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing proprioception: A critical review of methods. J Sport Health Sci. 2016;5:80-90.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: A reliability and validity study. PLoS One. 2015;10:e0140822.
- [CrossRef] [PubMed] [Google Scholar]
- Radiological and biochemical effects (CTX-II, MMP-3, 8, and 13) of low-level laser therapy (LLLT) in chronic osteoarthritis in Al-Kharj, Saudi Arabia. Lasers Med Sci. 2017;32:297-303.
- [CrossRef] [PubMed] [Google Scholar]
- High-intensity laser therapy on pain relief in symptomatic knee osteoarthritis: A systematic review and meta-analysis. J Back Musculoskelet Rehabil. 2023;36:1011-21.
- [CrossRef] [PubMed] [Google Scholar]
- Joint proprioception, muscle strength, and functional ability in patients with osteoarthritis of the knee. Arthritis Care Res. 2007;57:787-93.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the effect of high-intensity laser therapy (HILT) on function, muscle strength, range of motion, pain level, and femoral cartilage thickness in knee osteoarthritis: Randomized controlled study. Lasers Med Sci. 2023;38:218.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of tele-rehabilitation in patients with knee osteoarthritis: A randomized controlled trial. Digit Health. 2024;10:20552076241286186.
- [CrossRef] [PubMed] [Google Scholar]




