Translate this page into:
Epidemiology of surgically treated pelvis and acetabulum fractures in a Level-1 trauma centre in Oman
Corresponding Author:
Salim S Al Habsi
P. O. Box: 1490, Postal Code: 111, Muscat
Sultanate of Oman
drsalimalhabsi@hotmail.com
| How to cite this article: Al Habsi SS, Al Busaidi AH, Ghosh S, Shahin M, Luthra JS. Epidemiology of surgically treated pelvis and acetabulum fractures in a Level-1 trauma centre in Oman. J Musculoskelet Surg Res 2021;5:46-50 |
Abstract
Objective: The purpose of this study is to analyze the epidemiological characteristics of operated pelvic and acetabular fractures at our institution and to compare them with epidemiological data from different parts of the world. Methods: This is a retrospective study of trauma data at Khoula Hospital from January 2010 to December 2016. Epidemiological data including age, gender, mode of trauma, presence of injuries, fracture classification, surgical approach, and associated complications were analyzed. Results: A total of 209 patients with a diagnosis of pelvis and acetabular fracture were included in this study. Young age group (mean: 35) and male gender (68%) were predominately affected. The main leading cause of the injury was road traffic accidents (96%). There were a total of 179 (86%) acetabular fractures and 30 (14%) pelvic fractures. Fracture of the posterior wall of the acetabulum was the most common pattern (39%), followed by transverse fracture (27%). Anterior–posterior compression type was clearly the most common type of pelvis fracture (40%). Six patients had postoperative sciatic nerve palsy, five patients had venous thromboembolism, and nine patients had wound infection. Conclusion: The great majority of the patients were victims of road traffic accidents, male, and young adults. The posterior wall fracture was the most common pattern, as shown in other studies as well. However, we identified some epidemiological differences in comparison with some studies from some other parts of the world. These include a higher contribution of road traffic accidents as a mode of injury and a high female-to-male ratio.
Introduction
Pelvic–acetabular fractures constitute one of the major orthopedic injuries resulting from high-energy trauma.[1],[2] They are one of the most challenging musculoskeletal injuries, which require special attention for surgical treatment, including specialized hospitals and expertise. Road traffic accidents (RTA) are reported as the major cause of these catastrophic injuries.[1],[2],[3],[4],[5],[6],[7] There has been a decrease in the incidence of these fractures with improvement in protective legislations like enforcement of the seat belt use, the use of cars with airbags, use of speed radars, avoiding cell phone during driving, and improved safety measures at construction and worksite.[1],[5],[8],[9] The recent literature reports 37 pelvic fractures per 100,000 population annually, and 10% of them involve the acetabulum. Pelvic and acetabular fractures showed a bimodal age distribution, as they are common in the young population with high-energy trauma and in elderly people with osteoporosis. The epidemiology of acetabular fractures in Europe, the USA, Latin America, and East Asia has been well established; however, data from the Middle East countries are limited. Oman is undergoing fast economic development and growing population, with a high number of trauma cases encountered at different hospitals in the country. There is no previous local epidemiological study of such fractures conducted in Oman to the best of our knowledge. Khoula Hospital is the main trauma referral center in Oman, which deals with surgical treatment of pelvic and acetabular fractures. Most of the cases are transferred from different regional hospitals in the country for surgical stabilization of these fractures. Some studies revealed that acetabular fractures have different patterns between different parts of the world. For example, comparing the epidemiological profile and injury pattern of acetabular fractures between the USA and China showed differences in the mechanism of injury and age distribution.[8] The aim of this study was to make an epidemiological analysis of operated acetabular and pelvic fractures managed in Khoula Hospital, Oman, and to compare the results with epidemiological data from other parts of the world.
Methods
Data were collected retrospectively for 209 operated patients, who had presented to our hospital (including referred cases from peripheral hospitals) between January 2010 and December 2016 with a fracture of the pelvis and acetabulum. Age, gender, mechanism of trauma, associated injuries, fracture pattern, surgical approach, and associated complications were assessed. Data were collected from the hospital information system.
The Judet and Letournel classification system was used to group the fractures using anterior–posterior and oblique radiographs in addition to computed tomography scan.
We evaluated the available radiographs including immediate postoperative radiographs, at 6-week postoperative and at 3-month follow-up using Matta's radiological scoring to audit our results. We compared our descriptive data with some epidemiological studies conducted in different parts of the world.
Results
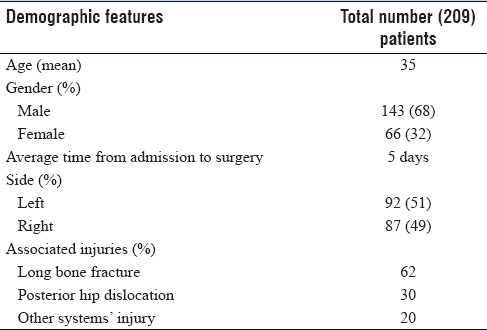
Of 209 operated patients included in this study, 179 patients had acetabular fractures and 30 patients had pelvic fractures. A total of 143 males were found in the study as opposed to 66 females giving a male-to-female ratio of 2.2:1. Ages ranged from 18 to 58 years, with a mean of 35 years. RTAs were the most frequent cause of trauma, responsible for 96% of the cases, followed by a fall from a height, which accounted for 4% of cases [Table - 1].
![[Table - 1]](#tbl_SaudiOrthopJ_2021_5_1_46_309271_t4.jpg){kind=link}
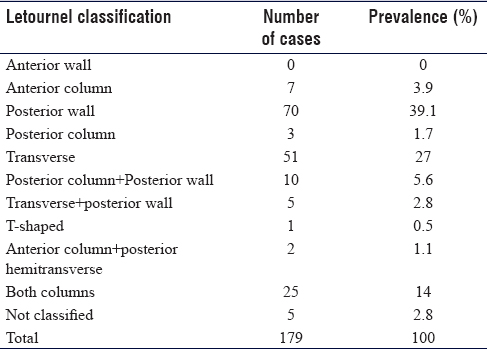
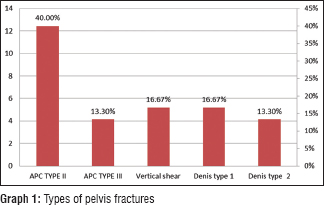
Fracture of the posterior wall of the acetabulum was the most frequent type seen in 39% of the cases, followed by a transverse fracture in 27% of the cases [Table - 2]. Anteroposterior compression Type II was clearly the most common type of pelvic fractures seen in 40% of the cases [Graph 1]. Around two-third (62%) of the patients had an associated long bone fracture (ipsilateral in 52% of the cases and the rest were contralateral). Injuries involving the chest, abdomen, maxillofacial, and spine were reported in 20% of the cases. Around one-third (35%) of patients had associated posterior dislocation of the hip.
![[Table - 2]](#tbl_SaudiOrthopJ_2021_5_1_46_309271_t5.jpg){kind=link}
All cases with acetabular fractures underwent open reduction and internal fixation (ORIF), with the mean time to operation after admission was 5 days. Kocher-Langenbeck approach was the most common approach used to fix the posterior wall and posterior column fractures [Figure - 1]. For anterior column and quadrilateral plate fractures, the most common approach utilized was the modified Stoppa approach. Except for a few cases, the majority of transverse and both column fractures underwent staged fixation, and the most displaced fracture was fixed first.
![[Figure - 1]](#fig_SaudiOrthopJ_2021_5_1_46_309271_f1.jpg){kind=link}
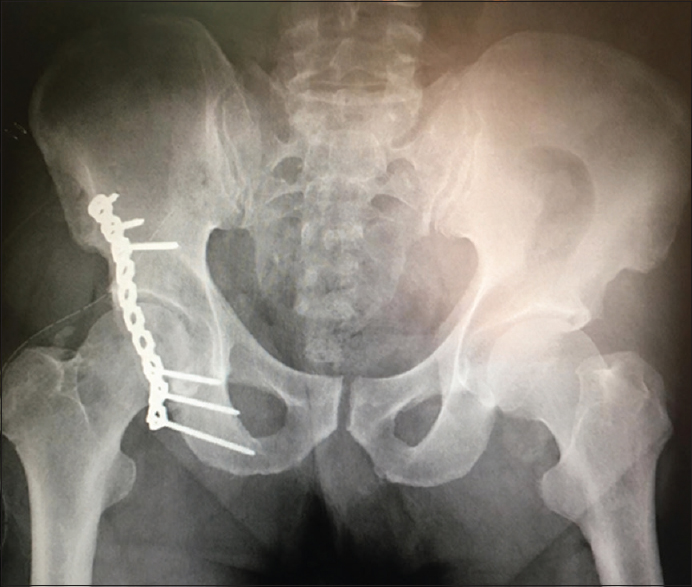 |
| Figure 1: Posterior wall acetabulum fracture fixed through Kocher Langenbeck approach |
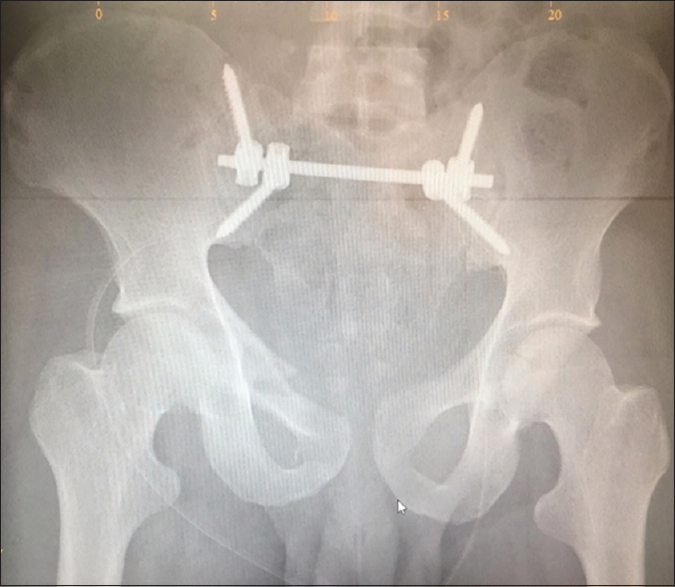
All cases of sacroiliac disruptions were fixed percutaneously with the help of intraoperative inlet and outlet views for the pelvis and true lateral view for the sacrum. Cases with pubic symphyseal diastasis were fixed using Pfannenstiel incision and anterior pelvic stabilization with reconstruction plates [Figure - 2]. For sacral fractures, the majority of the cases underwent ilioiliac fixation [Figure - 3]. Few cases of iliolumbar dissociation, which had associated fifth lumbar vertebra transverse process fracture underwent iliolumbar fixation.
![[Figure - 2]](#fig_SaudiOrthopJ_2021_5_1_46_309271_f2.jpg){kind=link}
![[Figure - 3]](#fig_SaudiOrthopJ_2021_5_1_46_309271_f3.jpg){kind=link}
 |
| Figure 2: Patient with pubic symphyseal diastasis fixed with reconstruction plate through Pfannenstiel incision |
 |
| Figure 3: A 40 years old male with Denis type-III sacral fracture fixed with ilioiliac fixation |
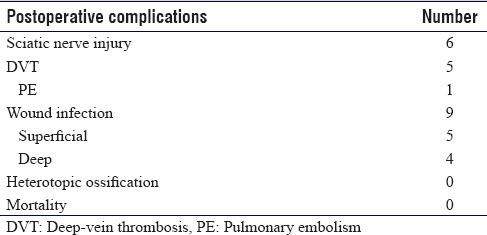
Six patients had postoperative sciatic nerve palsy, which had recovered over a period of time. Five patients had venous thromboembolism and one of them developed pulmonary embolism. Wound infection was reported in nine patients and in four cases, the infection was deep and required surgical debridement. In five cases, the wound infection was superficial and was treated with wound care and intravenous antibiotics. There were no cases of heterotopic ossification or reported postoperative mortality [Table - 3].
![[Table - 3]](#tbl_SaudiOrthopJ_2021_5_1_46_309271_t6.jpg){kind=link}
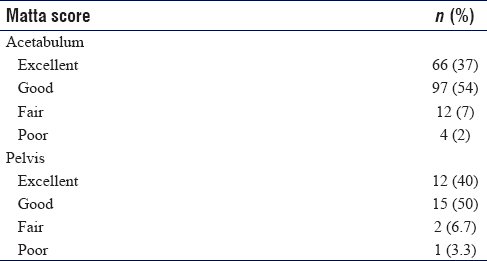
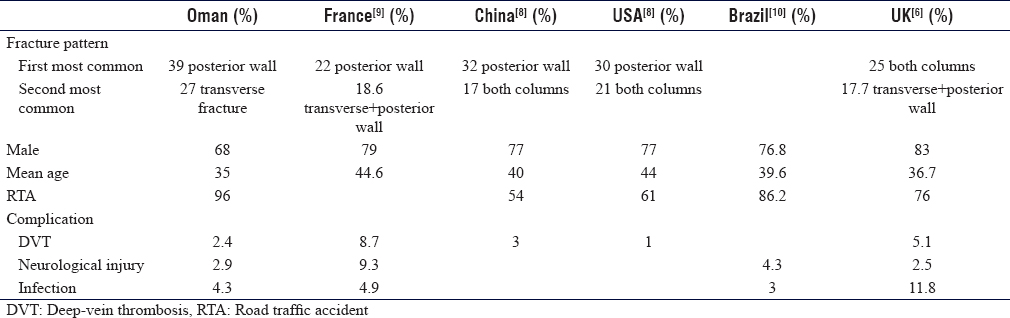
Matta's scoring results of our patients with acetabulum and pelvis fractures are highlighted in [Table - 4]. We compared our results with data from epidemiological studies conducted in some countries from different parts of the world [Table - 5].
![[Table - 4]](#tbl_SaudiOrthopJ_2021_5_1_46_309271_t7.jpg){kind=link}
![[Table - 5]](#tbl_SaudiOrthopJ_2021_5_1_46_309271_t8.jpg){kind=link}
Discussion
There is a lack of epidemiological data on acetabular and pelvic fractures in the Middle East, and to our best of knowledge, the recently reported study was from Qatar.[11]
Our results are inconsistent with other published epidemiological studies from different parts of the world in regard to mean age. In our series, we got a younger mean age group of 35 years with comparison to the average age of 47.3 years in Germany, 46.8–53.7 years in the UK, 39.6 years in Brazil, 40 years in the USA, and 44 years in China.[8],[10],[12],[13],[14] Unfortunately, this figure highlights the fact that the highest prevalence of this injury was among the socioeconomically and physically active populations.
RTAs are the main cause of acetabular fractures globally, and they account for 80.5% of the cases analyzed by Giannoudis et al.[12] In our series, RTAs were responsible for 96% of the cases, which is the highest contribution and percentage reported in the literature. RTA is a major public health problem in Oman. The rapid modernization and development in Oman's economy in the last years have changed many aspects of transportation in the country. The high number of RTAs in Oman is related to the expansion in the road networks accompanied by a rapid increase in the number of vehicles on the roads due to extensive growth and tremendous development in the country.
In our study, we found that the majority of the cases were male (68%). This finding was comparable to Giannoudis et al. who analyzed 3670 cases of displaced acetabular fractures and found that 69.4% of cases were male.[12] However, this figure is relatively lower than those reported in France, the USA, China, and Brazil, respectively 79%, 77%, 77%, and 76.8% males.[8],[9],[10] The lower number of falls from height in our study might explain the higher incidence of these fractures among females, with the fact that the majority of the workforce in Oman are male.
The prevalence of different fracture types in this study is almost consistent with that reported in other studies in regard to the most prevalent fracture pattern. In our series, posterior wall fracture was the most predominant fracture type reported in 39% of the cases, which correlate with other reports in literature like 22% in France, 32% in the USA, 30% in China, and 18.4% in Qatar.[8],[9],[11] However, in our series, we observed that transverse fracture is the second predominance fracture in 27% of the cases compared to 3.9% in France, 6% in the USA, 5% in China, and 4.9% in Qatar.[8],[9],[11] There was a much lower incidence of anterior column fractures in Oman as fall from height cases are less. In the present study, we found that Type B (rotationally unstable and vertically stable pelvic fractures) was the most common surgically treated pelvic injury followed by Type C fractures (rotationally and vertically unstable fractures), which is consistent with most studies in the literature.[15],[16],[17]
These fractures usually result from high-energy trauma and the majority of them have concomitant injuries. Extremity fractures and head injury are the commonly reported associated injuries. This is also evident in our study in which concomitant abdominal, chest, and head injuries were found to be present in 20% of the cases. However, the incidence of other associated orthopedic fractures was noted at 62% of all acetabular fracture cases in Oman. In our series, ORIF was used in all the patients. Kocher-Langenbeck approach was utilized most frequently in the surgical management of acetabular fractures. However, the modified Stoppa approach was used for fixation of the anterior column and quadrilateral plate fractures. Primary total hip replacement was not considered in our cases as the primary treatment of acetabular or pelvic fractures.
The average time between the trauma and the surgery was 5 days in our study compared to 8.9 ± 2.9 days in the meta-analysis by Giannoudis et al.[18]
In our cohort, we found that the lower sciatic nerve injury rate was only 3.4% (six cases) in comparison to 7.5 in Qatar and 7.8% in France.[9],[11] In all the cases, the deficit has recovered over a period of time.
The main advantage of this study is that it is considered the first epidemiological study of the surgically treated acetabular and pelvic fractures in Oman. Another advantage is the large sample size: to our best knowledge, this is the largest epidemiological study conducted in the Middle East.
The limitations of the current study are the retrospective design, which could have the potential of missing information. The follow-up period was short and late complications like osteoarthritis or avascular necrosis were not recorded. In addition, we only included cases which were treated surgically as conservatively managed fractures are not recorded in our computer database. Finally, only an objective assessment tool was used to assess our surgical results.
Conclusion
We observed that the great majorities of the operated acetabular and pelvic fracture patients in Oman were due to RTAs, males, in the economically active age group. The posterior wall of the acetabulum was fractured in the majority of the patients, in agreement with previously published articles. However, in our sample, we recorded the highest contribution of RTAs as a mode of injury, high female-to male–ratio, and high prevalence of transverse acetabular fracture.
Recommendations
As the RTAs are significantly the main cause of acetabulum and pelvis fracture in the country, we feel that the awareness of public and road users to respect safety standards and the development of a traffic accident prevention policy and legislation are essentials. Future multicenter prospective studies are also recommended.
Ethical consideration
Ethical approval was obtained from the Khoula Hospital Research Ethical Committee (PRO042020057). April 28, 2020.
Financial support and sponsorship
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
There are no conflicts of interest
Authors' contributions
SAH conceived and designed the article's outlines and prepared the initial and final draft. ASB contributed with draft writing and data collection and obtained the ethical approval. SOG designed the study and data collection and interpretation. MAS contributed to data collection, analysis, and study design. JSL suggested the idea of the study and reviewed the final manuscript. All the authors have critically reviewed and approved the final draft and are responsible for the manuscript's content and similarity index.
| 1. | Laird A, Keating JF. Acetabular fractures: A 16-year prospective epidemiological study. J Bone Joint Surg Br 2005;87:969-73. [Google Scholar] |
| 2. | Letournel E. Acetabulum fractures: classification and management. Clin Orthop 1980:81-106. [Google Scholar] |
| 3. | Moed BR, Carr SE, Watson JT. Open reduction and internal fixation of posterior wall fractures of the acetabulum. Clin Orthop 2000;(377):57–67. [Google Scholar] |
| 4. | Blum J, Beyermann K, Ritter G. Incidence of acetabular fractures before and after introduction of compulsory seatbelt fastening. Unfallchirurgie 1991;17:274-9. [Google Scholar] |
| 5. | Al-Qahtani S, O'Connor G. Acetabular fractures before and after the introduction of seatbelt legislation. Can J Surg 1996;39:317-20. [Google Scholar] |
| 6. | Madhu R, Kotnis R, Al-Mousawi A, Barlow N, Deo S, Worlock P, et al. Outcome of surgery for reconstruction of fractures of the acetabulum. The time dependent effect of delay. J Bone Joint Surg Br 2006;88:1197-203. [Google Scholar] |
| 7. | Liebergall M, Mosheiff R, Low J, Goldvirt M, Matan Y, Segal D. Acetabular fractures. Clinical outcome of surgical treatment. Clin Orthop 1999:205-16. [Google Scholar] |
| 8. | Mauffrey C, Hao J, Cuellar DO 3rd, Herbert B, Chen X, Liu B, et al. The epidemiology and injury patterns of acetabular fractures: Are the USA and china comparable? Clin Orthop Relat Res 2014;472:3332-7. [Google Scholar] |
| 9. | Boudissa M, Francony F, Kerschbaumer G, Ruatti S, Milaire M, Merloz P, et al. Epidemiology and treatment of acetabular fractures in a level-1 trauma centre: Retrospective study of 414 patients over 10 years. Orthop Traumatol Surg Res 2017;103:335-9. [Google Scholar] |
| 10. | Dias MV, Goldsztajn F, Guimarães JM, Grizendi JA, Correia M, Rocha TH, et al. Epidemiology of acetabulum fractures treated at the instituto nacional de traumatologia E ortopedia (INTO). Rev Bras Ortop 2010;45:474-7. [Google Scholar] |
| 11. | Ahmed M, Abuodeh Y, Alhammoud A, Salameh M, Hasan K, Ahmed G, et al. Epidemiology of acetabular fractures in qatar. Int Orthop 2018;42:2211-7. [Google Scholar] |
| 12. | Giannoudis PV, Grotz MR, Tzioupis C, Dinopoulos H, Wells GE, Bouamra O, et al. Prevalence of pelvic fractures, associated injuries, and mortality: The United Kingdom perspective. J Trauma 2007;63:875-83. [Google Scholar] |
| 13. | Ochs BG, Marintschev I, Hoyer H, Rolauffs B, Culemann U, Pohlemann T, et al. Changes in the treatment of acetabular fractures over 15 years: Analysis of 1266 cases treated by the German Pelvic Multicentre Study Group (DAO/DGU). Injury 2010;41:839-51. [Google Scholar] |
| 14. | Kumar A, Shah NA, Kershaw SA, Clayson AD. Operative management of acetabular fractures. A review of 73 fractures. Injury 2005;36:605-12. [Google Scholar] |
| 15. | Grotz MR, Allami MK, Harwood P, Pape HC, Krettek C, Giannoudis PV, et al. Open pelvic fractures: Epidemiology, current concepts of management and outcome. Injury 2005;36:1-3. [Google Scholar] |
| 16. | Gänsslen A, Pohlemann T, Paul C, Lobenhoffer P, Tscherne H. Epidemiology of pelvic ring injuries. Injury 1996;27 Suppl 1:S-A13-20. [Google Scholar] |
| 17. | Pereira GJ, Damasceno ER, Dinhane DI, Bueno FM, Leite JB, Ancheschi BD, et al. Epidemiology of pelvic ring fractures and injuries. Rev Bras Ortop 2017;52:260-9. [Google Scholar] |
| 18. | Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum. A meta-analysis. J Bone Joint Surg Br 2005;87:2-9. [Google Scholar] |
Fulltext Views
3,195
PDF downloads
1,441




