Translate this page into:
Evaluation of radiation exposure from X-ray imaging among scoliotic patients at a tertiary care hospital
2 King Abdullah International Research Medical Center; College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
3 King Abdullah International Medical Research Center, Population Health Research Section, Riyadh, Saudi Arabia
Corresponding Author:
Ibrahim A Almohini
College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Ar Rimayah, Riyadh 14611
Saudi Arabia
dr.ibrahimalmohini@gmail.com
| How to cite this article: Konbaz F, Alhandi AA, Almohini IA, Almubarak AK, Alamri N, Ghazal HS. Evaluation of radiation exposure from X-ray imaging among scoliotic patients at a tertiary care hospital. J Musculoskelet Surg Res 2021;5:41-45 |
Abstract
Objectives: The radiographs were reported to cause a potential risk of cancer resulting from multiple spinal radiographs' cumulative radiation. Based on the spine's anatomic location, covering a large body area and its proximity to radiosensitive organs, the radiation dose required is relatively higher than annual background radiation ~2.4 millisievert (mSv)/year. The aim of the study was to estimate the radiation doses from imaging in scoliotic patients at a tertiary care hospital. Methods: The study design was a retrospective cohort study where the charts of scoliotic patients aged 12 years and older were reviewed between 2008 and 2017. Evaluation of the spinal imaging was commenced at the time of diagnosis, where the patients were initially seen in the orthopedic clinic with a follow-up period of 2 years. The estimated radiation dose was measured according to the average effective dose by mSv. Results: The total sample size was 140 patients, and the mean age was 19.3 years. Idiopathic scoliosis was the main subtype with 116 patients (82.6%). The average of total spine X-ray films was 5.2. The average cumulative effective radiation dose was estimated at 22.13 mSv. The initial management type was found to have a significant linear effect (P < 0.0001) on the cumulative effective radiation dose. Conclusions: The cumulative radiation dose is markedly elevated in comparison to the reported numbers in the literature (yearly average dose = 2.17–15.07 mSv). Ultra-low-dose radiation may need to be used instead of standard radiographs to reduce radiation risk.
Introduction
The incidence of scoliosis among adults is a source of debate with a wide range of 1.4%–32%.[1],[2],[3],[4] The most common scoliotic disorder, adolescent idiopathic scoliosis (AIS), happens during adolescent years, with a prevalence of 2%–3%.[1] AIS is described as a lateral curvature of the spine, which is accompanied by rotational malalignment.[1] The etiology is thought to be secondary to genetic factors, but the exact mechanism for an abnormal curve's appearance is unknown.[1],[5]
Along with the clinical assessment, X-ray imaging is utilized to guide the management, either the surgical or nonsurgical treatment, and track abnormal curve angle progression.[6] The imaging procedures performed for spinal deformities such as scoliosis were reported to cause a potential risk of cancer resulting from cumulative radiation dose.[7],[8],[9] Furthermore, the lifetime risk of breast cancer and inherited genetic mutations among scoliotic patients who underwent multiple spinal radiographs is estimated to be 2% and 3%, respectively.[7],[8],[9]
Ionizing radiation is considered a carcinogen.[10] Exposure to ionizing radiation places individuals at high risk of complications, including thyroid cancer, leukemia, cataract, and skin erythema.[10]
Multiple studies revealed that whole-spine radiography carries the highest radiation risk.[11],[12] Based on the anatomic location of the spine, covering a large body area and its proximity to radiosensitive organs, the radiation dose required is relatively high, which inherently increases the risk of malignancy.[13] The body tissues of the pediatric age group are known to have high radiosensitivity and more prone to damage by radiation due to their lifetime radiation exposure being relatively longer than adults.[14] Moreover, females tend to have a higher overall risk of cancer compared to males with the same whole-spine radiography.[11],[12],[13]
The aim of the study was to estimate the cumulative effective radiation doses from imaging in scoliotic patients at a tertiary care hospital. The cumulative radiation dose is defined as the total ionizing radiation from spine films received by the patient over a specific time period. The authors hypothesized that scoliotic patients are exposed to an above average dosage of radiation, with the average being 0.170–1.090 millisievert (mSv) from spine radiographs.[14] Furthermore, the study aimed to provide information for future practice guidance concerning spinal deformity and radiation exposure. Awareness of patients and families about cumulative radiation dose may relieve their worry regarding possible risks and involve them in their management plan.
Materials and Methods
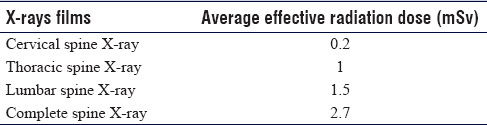
The study design was a retrospective chart review study. Charts of scoliotic patients aged 12 years and older between 2008 and 2017 were reviewed. The spinal imaging evaluation was commenced from the time of diagnosis, where the patients were initially seen in the orthopedic clinic. The follow-up period of radiation exposure involved 2-year period. Any patient diagnosed with degenerative scoliosis was excluded. Radiation dosages of other imaging procedures, such as computed tomography scan and intraoperative fluoroscopy, were not calculated. The X-ray machine utilized for spine films in the study was a digital X-ray with an auto-image pasted technique that recruits multiple images via a detector spanning upper to lower spine segments. The estimation of cumulative radiation was measured according to the values of the average effective doses for each spine X-ray film by mSv observed in the literature [Table - 1].[15],[16] The average dose was calculated using midpoint values from the literature where the digits rounded to one decimal place after an integer number. The effective dose is a valuable measure useful to calculate the amount of whole radiation absorbed by each organ in the body.[17],[18] The categorical parameters such as gender, scoliosis subtypes, anatomic location of spine deformity, and type of deformity treatment were gathered. The collected numerical parameters also involve age, body mass index, Cobb angle, number of spine radiographs, and effective radiation dose from radiological procedures. The sample size was calculated by Rasoft, Inc. with a 5% margin of error and a 95% confidence interval based on Dr. Alshami's study (prevalence of spinal disorders is 28.1%).[19] The estimated sample size is 295. The data were compiled on a Microsoft Excel sheet and then uploaded into SAS software (SAS Institute Inc., NC, USA). Descriptive analysis was carried out by calculating the frequencies and percentages for categorical variables, means, and medians for continuous variables. A general linear model (GLM) or analysis of variance was used to assess between- and within-group significances and post hoc analysis was done to make group comparison for the mean radiation dose, and P < 0.05 was assumed as statistically significant with 95% confidence level. All the statistical analyses were done using SAS software (SAS Institute Inc., NC, USA).
![[Table - 1]](#tbl_SaudiOrthopJ_2021_5_1_41_309270_t1.jpg){kind=link}
Results
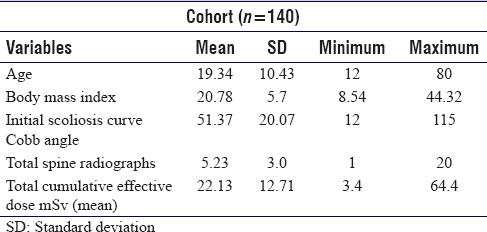
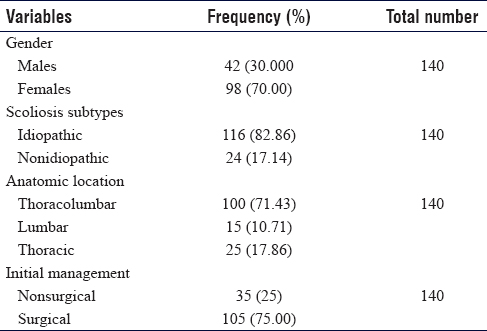
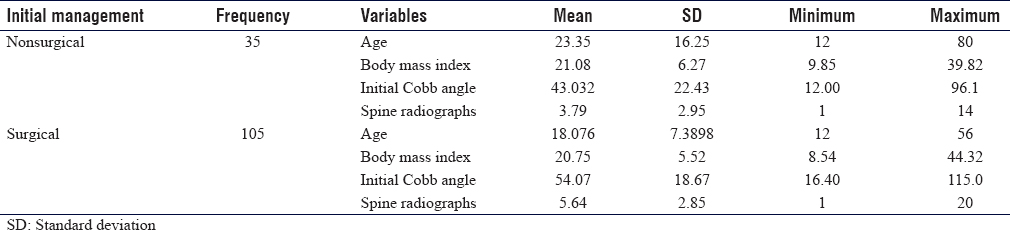
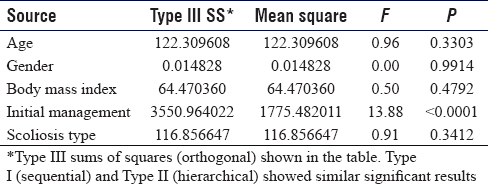
Of 219 patients, the total sample size in this study was 140 patients with complete follow-up and no missed data. The mean age was 19.3 years. Females formed most of the sample, counting for 98 patients (70%), and AIS was the main subtype with 116 patients (82.6%). The mean initial Cobb angle at the time of diagnosis was 51.3°, and the average number of total spine X-ray films was found to be 5.2. The average cumulative effective radiation dose was estimated at 22.13 mSv [Table - 2] and [Table - 3]. Moreover, the mean number of spine X-ray films among a nonsurgical group found to be 3.79, whereas the surgical group had a mean of spine X-ray films estimated as 5.64 [Table - 4]. Four cases were diagnosed with spondylolisthesis and underwent surgical intervention. Moreover, 91 patients (65%) with AIS underwent corrective surgery. Among the tested independent variables, the type of initial management (whether surgical or nonsurgical) was found to have a significant linear effect (P < 0.0001) on the cumulative effective radiation dose mean through the GLM univariate procedure [Table - 5].
![[Table - 2]](#tbl_SaudiOrthopJ_2021_5_1_41_309270_t2.jpg){kind=link}
![[Table - 3]](#tbl_SaudiOrthopJ_2021_5_1_41_309270_t3.jpg){kind=link}
![[Table - 4]](#tbl_SaudiOrthopJ_2021_5_1_41_309270_t4.jpg){kind=link}
![[Table - 5]](#tbl_SaudiOrthopJ_2021_5_1_41_309270_t5.jpg){kind=link}
Discussion
Spinal radiography in scoliosis patients is important in diagnosis and management. In fact, the definition of scoliosis needs to meet the radiographic measurements on a radiograph. The curvature in the coronal plane of at least 10° (Cobb angle) with a rotation of the involved vertebrae. X-ray imaging remains an essential part of diagnosing a spine deformity despite the presence of advanced new techniques. The significance of the radiation dose imparted by spine radiographs is still underestimated among the physicians in current practice in terms of the benefit and risk the patients are gaining over their follow-up period. To perform appropriate risk-benefit analyses of current imaging practices, it is imperative that the amount of radiation received by radiographs be accurately quantified. Our study's cumulative mean effective radiation dose was 22.13 mSv that is 9 folds higher than the mean effective cumulative dose from background radiation, which is originated from environmental sources and estimated as ~2.4 mSv/year.[20] The same finding is supported by another study from Xie En where the scoliosis ionizing radiation from computed tomography scan over 11 years was three times greater than annual background radiation.[21] Another study from Law et al. investigated the cumulative effective dose of annual spine radiography among scoliotic patients aged 5 years up to 30 years that was reported as 15 mSv.[14] It is noted that in reported studies, a standardized method is lacking in terms of inclusion criteria. The ionizing radiation that is found significantly high in our study could be referred to a high mean of Cobb angle at the diagnosis (51.37°) and significant complexity during clinical evaluation time. The significant finding of linear regression for initial management effect on cumulative effective dose can be explained to the majority of gathered samples undergoing surgical management, which requires close postoperative follow-up with further radiological examinations. One of the best strategies to minimize radiation exposure is to apply the as low as reasonably achievable principle, which is particularly important among pediatric age groups as their body organs are more prone to carcinogenesis and their risk to radiation exposure is longer during their early lifetime.[22] Improvement in nonionizing radiation-based imaging techniques such as magnetic resonance imaging widely replaces ionizing radiation for assessment of bony anatomy and may lead to the complete dependence for diagnostic purposes.[23] Furthermore, modern X-ray machines such as the EOS™ X-ray machine provide marked advancement in imaging systems by allowing anterior-posterior and lateral views of the whole body to be captured simultaneously in an upright position and construct a three-dimensional model using slot-scanning systems that offer very minimal radiation exposure. It also provides a high-quality image performed by single exposure that takes 20 s with less examination time in contrast to a conventional X-ray machine that requires multi-exposure and more radiation risk. The created image has a scale ratio of 1:1 with physical reality and true to object equality.[23],[24] Another way to reduce the radiation burden found in the literature is by changing the image orientation shown in the posterior-anterior view, which is found to carry much less radiation in comparison to the anterior-posterior view for spine-related imaging.[25],[26] Lack of actual values of radiation dose from this X-ray machines to reflect the standard programmed amount of various spine X-ray radiations is considered a potential weakness in the study due to its retrospective design and the inability of the machine to obtain real-time dose estimation as it is traditionally manufactured providing only real-time dose not being retrieved. However, it is worth to note that relying on the average radiation doses from literature allowed to represent a distinct finding of significant radiation exposure in this study. Future studies are encouraged to explore the safety of more advanced radiation machines.
Conclusions
Cumulative effective radiation dose in the study is markedly elevated in comparison to the reported numbers in the literature, which requires implementing methods to reduce their frequency. We believe that a high dose of radiation in this study is due to cases' complexity from a high value of the Cobb angle, which necessitates repetitive radiation exposures during the follow-up period.
Recommendation
Further studies with several hospitals and a wider number of scoliotic patients under numerous geographic regions are needed to perform the cost analysis evaluating the financial consumption of such frequent spine X-ray radiation among scoliotic patients.
Ethical approval
The research was conducted after acquiring approval from the Institutional Review Board of King Abdullah International Medical Research Center, Riyadh, dated January 12, 2019, study reference number: IRBC/0130/19. The data were collected by the research team members only via a computer, which was fully secured with a password to keep the patients' data safe. The principal investigator assured that privacy and confidentiality were protected; no identifiers or personal information were collected and all data were kept in a secured place within institution premises, both hard and soft copies.
Acknowledgment
The authors would like to thank Majd Abdulrahman Binkhunain, Meshail Saleh Alkhaleel, and Rema Ibraheem Alshagary for their contribution to data collection.
Financial support and sponsorship
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
There are no conflicts of interest.
Authors' contribution
FMK conceived and supervised the study. AAH, IAM, and HSG conducted the study and wrote the initial draft. IAM collected and organized the data. AAH and AM interpreted and analyzed the data. IAM and NA wrote and prepared the final draft. All authors have critically reviewed and approved the final draft and are responsible for the manuscript's content and similarity index.
| 1. | Hershkovich O, Friedlander A, Gordon B, Arzi H, Derazne E, Tzur D, et al. Association between body mass index, body height, and the prevalence of spinal deformities. Spine J 2014;14:1581-7. [Google Scholar] |
| 2. | Carter OD, Haynes SG. Prevalence rates for scoliosis in US adults: Results from the first national health and nutrition examination survey. Int J Epidemiol 1987;16:537-44. [Google Scholar] |
| 3. | Francis RS. Scoliosis screening of 3,000 college-aged women. The Utah Study--Phase 2. Phys Ther 1988;68:1513-6. [Google Scholar] |
| 4. | Biot B, Perdrix D. Frequence de la scoliose lombaire a l'age adulte. Ann Med Phys 1982;25:251-4. [Google Scholar] |
| 5. | Noshchenko A, Hoffecker L, Lindley EM, Burger EL, Cain CM, Patel VV, et al. Predictors of spine deformity progression in adolescent idiopathic scoliosis: A systematic review with meta-analysis. World J Orthop 2015;6:537-58. [Google Scholar] |
| 6. | Bussieres A, Taylor J, Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults-an evidenced-based approach – Part 3: Spinal disorders. J Manip Physiol Ther 2008;31:33-88. [Google Scholar] |
| 7. | Doody MM, Lonstein JE, Stovall M, Hacker DG, Luckyanov N, Land CE. Breast cancer mortality after diagnostic radiography: Findings from the U.S. scoliosis cohort study. Spine (Phila Pa 1976) 2000;25:2052-63. [Google Scholar] |
| 8. | Hui SC, Pialasse JP, Wong JY, Lam TP, Ng BK, Cheng JC, et al. Radiation dose of digital radiography (DR) versus micro-dose x-ray (EOS) on patients with adolescent idiopathic scoliosis: 2016 SOSORT- IRSSD “John Sevastic Award” winner in imaging research. Scoliosis Spinal Disord 2016;11:46. [Google Scholar] |
| 9. | Levy AR, Goldberg MS, Hanley JA, Mayo NE, Poitras B. Projecting the lifetime risk of cancer from exposure to diagnostic ionizing radiation for adolescent idiopathic scoliosis. Health Phys 1994;66:621-33. [Google Scholar] |
| 10. | Srinivasan D, Than KD, Wang AC, La Marca F, Wang PI, Schermerhorn TC, et al. Radiation safety and spine surgery: Systematic review of exposure limits and methods to minimize radiation exposure. World Neurosurg 2014;82:1337-43. [Google Scholar] |
| 11. | Simpson AK, Whang PG, Jonisch A, Haims A, Grauer JN. The radiation exposure associated with cervical and lumbar spine radiographs. J Spinal Disord Tech 2008;21:409-12. [Google Scholar] |
| 12. | Newton PO, Khandwala Y, Bartley CE, Reighard FG, Bastrom TP, Yaszay B. New EOS imaging protocol allows a substantial reduction in radiation exposure for scoliosis patients. Spine Deform 2016;4:138-44. [Google Scholar] |
| 13. | Hwang YS, Lai PL, Tsai HY, Kung YC, Lin YY, He RJ, et al. Radiation dose for pediatric scoliosis patients undergoing whole spine radiography: Effect of the radiographic length in an auto-stitching digital radiography system. Eur J Radiol 2018;108:99-106. [Google Scholar] |
| 14. | Law M, Ma WK, Lau D, Chan E, Yip L, Lam W. Cumulative radiation exposure and associated cancer risk estimates for scoliosis patients: Impact of repetitive full spine radiography. Eur J Radiol 2016;85:625-8. [Google Scholar] |
| 15. | Jenkins HJ, Downie AS, Moore CS, French SD. Current evidence for spinal X-ray use in the chiropractic profession: A narrative review. Chiropr Man Therap 2018;26:48. [Google Scholar] |
| 16. | Mettler FA Jr, Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: A catalog. Radiology 2008;248:254-63. [Google Scholar] |
| 17. | Jacobi W. The concept of the effective dose – A proposal for the combination of organ doses. Radiat Environ Biophys 1975;12:101-9. [Google Scholar] |
| 18. | McCollough CH, Schueler BA. Calculation of effective dose. Med Phys 2000;27:828-37. [Google Scholar] |
| 19. | Alshami AM. Prevalence of spinal disorders and their relationships with age and gender. Saudi Med J 2015;36:725-30. [Google Scholar] |
| 20. | United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) Sources and effects of ionizing radiation. UNSCEAR 2000 Report to the General Assembly, with scientific annexes, Volume I: Sources Vol. E.00.IX.3. New York: United Nations; 2000. p. 1-654. [Google Scholar] |
| 21. | En X. P95. Radiation exposure during the course of treatment for early-onset scoliosis: Longitudinal pilot study. The Spine J 2019;19:S202-3. [Google Scholar] |
| 22. | Goldberg MS, Mayo NE, Levy AR, Scott SC, Poîtras B. Adverse reproductive outcomes among women exposed to low levels of ionizing radiation from diagnostic radiography for adolescent idiopathic scoliosis. Epidemiology 1998;9:271-8. [Google Scholar] |
| 23. | Deschênes S, Charron G, Beaudoin G, Labelle H, Dubois J, Miron MC, et al. Diagnostic imaging of spinal deformities: Reducing patients radiation dose with a new slot-scanning X-ray imager. Spine (Phila Pa 1976) 2010;35:989-94. [Google Scholar] |
| 24. | Illés T, Somoskeöy S. The EOS™ imaging system and its uses in daily orthopaedic practice. Int Orthop 2012;36:1325-31. [Google Scholar] |
| 25. | Luo TD, Stans AA, Schueler BA, Larson AN. Cumulative Radiation exposure with EOS imaging compared with standard spine radiographs. Spine Deform 2015;3:144-50. [Google Scholar] |
| 26. | Levy AR, Goldberg MS, Mayo NE, Hanley JA, Poitras B. Reducing the lifetime risk of cancer from spinal radiographs among people with adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 1996;21:1540-7. [Google Scholar] |
Fulltext Views
4,892
PDF downloads
1,882




