Translate this page into:
Intracapsular osteochondroma of the humeral head in a skeletally mature patient: A rare cause for restriction in the range of movement
Corresponding Author:
Reddy Ravikanth
Department of Radiology, Holy Family Hospital, Thodupuzha - 685 605, Kerala
India
ravikanthreddy06@gmail.com
| How to cite this article: Ravikanth R, Kamalasekar K. Intracapsular osteochondroma of the humeral head in a skeletally mature patient: A rare cause for restriction in the range of movement. J Musculoskelet Surg Res 2019;3:235-236 |
Dear Editor,
We present a rare case of restricted shoulder motion due to a benign osteochondroma from the humeral head in a skeletally mature individual.
A 61-year-old male patient presented with a progressive onset of pain in the left shoulder for 4 months with restriction of shoulder movements, particularly external rotation, forward elevation, and abduction. The tests for impingement and rotator cuff injuries were negative. Magnetic resonance imaging (MRI) revealed the presence of a lobulated bony outgrowth measuring 2.1 cm × 1.6 cm arising from the posterior humeral head and extending into the axillary pouch [Figure - 1]. The bony outgrowth demonstrated continuity with the bony cortex and medullary canal of the humeral head with a cartilage cap measuring 3.3 mm on T2-weighted images [Figure - 2]. The patient underwent posterior approach surgery, which was by passing through the interval between the infraspinatus and teres minor muscles, and the lesion was completely excised. The lesion had a lobulated appearance and a cartilage cap without signs of necrosis. Histopathology confirmed the diagnosis as benign osteochondroma with no features of malignant transformation [Figure - 3]. After resection, the patient had an uneventful recovery and regained normal function of the right shoulder joint. He had the range of motion recovered to 155° in a 3-month time, and he has remained asymptomatic without any complications.
![[Figure - 1]](#fig_SaudiOrthopJ_2019_3_2_235_250795_f1.jpg){kind=link}
![[Figure - 2]](#fig_SaudiOrthopJ_2019_3_2_235_250795_f2.jpg){kind=link}
![[Figure - 3]](#fig_SaudiOrthopJ_2019_3_2_235_250795_f3.jpg){kind=link}
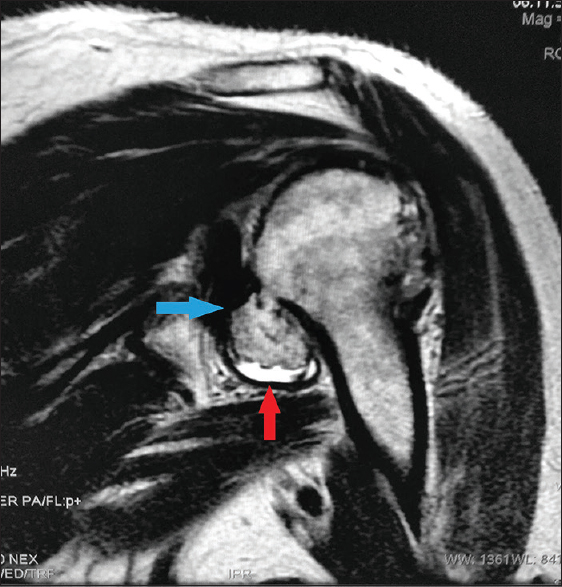 |
| Figure 1: Coronal T2-weighted magnetic resonance image demonstrating cartilage cap of humeral head osteochondroma (red arrow) and its proximity to the glenoid (blue arrow). Note the well-maintained cortical continuity of osteochondroma in the region of the cartilage cap |
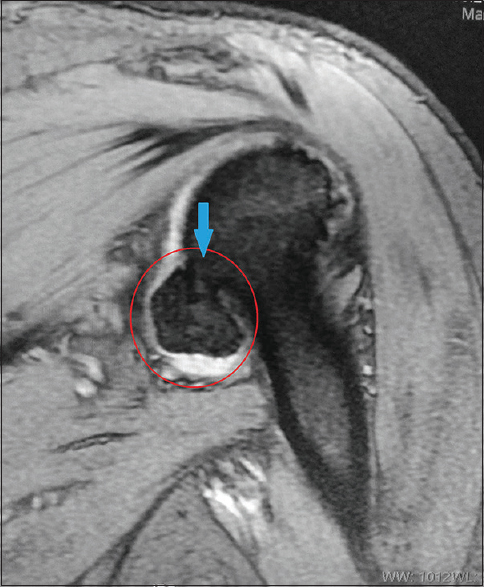 |
| Figure 2: Coronal MERGE (gradient) magnetic resonance image demonstrating an expansion of the axillary recess by the mass (circle) causing restriction of forward elevation and abduction in a skeletally mature elderly patient. Note the medullary continuity between the osteochondroma and host humeral head (blue arrow) |
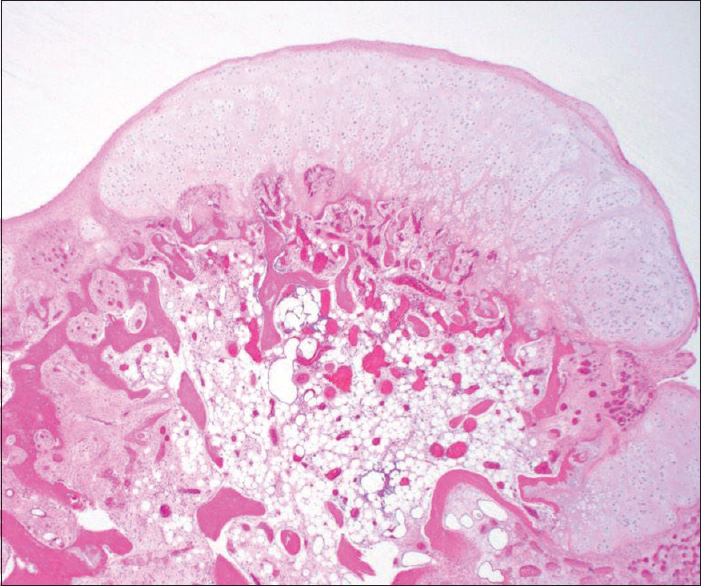 |
| Figure 3: The histologic examination shows the cortex, bone marrow space, and cartilage cap. There is no evidence of malignancy (H and E, ×40) |
Solitary osteochondroma as an entity is described as osteochondromatous exostosis, with the long bones of the lower limbs most commonly affected.[1] The proximal portion of femur and humerus are preferentially affected.[2] Osteochondromas usually affect immature skeleton, growing slowly and progressively with the bone involved causing complications of mechanical origin, and the growth stops when skeletal maturity is attained. In the pedunculated type of osteochondromas, acute-onset pain occurs secondary to local trauma, causing fracture of the base of peduncle.[3] Continuing growth of the lesion after skeletal maturity is suspicious for malignant sarcomatous transformation.[4] In intracapsular osteochondroma of the humeral head, the limited range of movement might be due to the expansion of the lobulated mass into the axillary recess creating excess tension causing limitation in movements such as forward elevation and abduction. Direct impingement of the osteochondroma with the glenoid during external rotation could also be a possible mechanism for limiting the range of movement. MRI demonstrates cortical and medullary continuity between the exostosis and the parent bone. The thickness of the cartilage cap on MRI is used as a criterion in differentiating benign osteochondroma from malignant sarcomatous transformation.[5] Cartilage cap thickness measuring more than 1.5–2.0 cm may be indicative of malignant transformation.[6] The cartilage thickness may be naturally thicker than skeletally mature skeleton and may reach more than 3.0 cm in children.[7] Clinical symptoms of pain and impression of a growing mass of the around the shoulder should alert potential risk of malignant transformation of an osteochondroma. Functional impairment, pain, and fractured base of pedunculated osteochondroma may be indications of surgery in solitary osteochondroma. Wide surgical resection is practiced in cases of malignant transformation.[8] Complications of solitary osteochondromas include fracture base of pedunculated lesion, pseudoaneurysm formation, capsulitis and bursitis, neurological complications, and sarcomatous transformation, which is rarely occurring in <1% of patients.[9] In conclusion, we presented a rare cause of limited range of motion in a skeletally mature individual with osteochondroma involving the humeral head who later underwent surgery with subsequent improvement in the range of motion.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. | de Souza AM, Bispo Júnior RZ. Osteochondroma: Ignore or investigate? Rev Bras Ortop 2014;49:555-64. [Google Scholar] |
| 2. | Scarborough MT, Moreau G. Benign cartilage tumors. Orthop Clin North Am 1996;27:583-9. [Google Scholar] |
| 3. | Padua R, Castagna A, Ceccarelli E, Bondì R, Alviti F, Padua L, et al. Intracapsular osteochondroma of the humeral head in an adult causing restriction of motion: A case report. J Shoulder Elbow Surg 2009;18:e30-1. [Google Scholar] |
| 4. | Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar] |
| 5. | Karasick D, Schweitzer ME, Eschelman DJ. Symptomatic osteochondromas: Imaging features. AJR Am J Roentgenol 1997;168:1507-12. [Google Scholar] |
| 6. | Lee JK, Yao L, Wirth CR. MR imaging of solitary osteochondromas: Report of eight cases. AJR Am J Roentgenol 1987;149:557-60. [Google Scholar] |
| 7. | De Beuckeleer LH, De Schepper AM, Ramon F. Magnetic resonance imaging of cartilaginous tumors: Is it useful or necessary? Skeletal Radiol 1996;25:137-41. [Google Scholar] |
| 8. | Mehta M, White LM, Knapp T, Kandel RA, Wunder JS, Bell RS, et al. MR imaging of symptomatic osteochondromas with pathological correlation. Skeletal Radiol 1998;27:427-33. [Google Scholar] |
| 9. | Woertler K, Lindner N, Gosheger G, Brinkschmidt C, Heindel W. Osteochondroma: MR imaging of tumor-related complications. Eur Radiol 2000;10:832-40. [Google Scholar] |
Fulltext Views
3,588
PDF downloads
550




