
Translate this page into:
Low trochanteric fractures in the presence of knee arthroplasty: The role of intermediate length cephalomedullary nail
 MD, Sarah Hine1MD, Kenneth B. Sams1BA, Abigail Nye1BS, Michael Suk1MD, Daniel S. Horwitz1MD
MD, Sarah Hine1MD, Kenneth B. Sams1BA, Abigail Nye1BS, Michael Suk1MD, Daniel S. Horwitz1MD
*Corresponding author: Ahmed Nageeb Mahmoud, Department of Orthopedic Surgery, Geisinger Medical Center, Danville, Pennsylvania, United States. amahmoud@geisinger.edu
-
Received: ,
Accepted: ,
How to cite this article: Mahmoud AN, Hine S, Sams KB, Nye A, Suk M, Horwitz DS. Low trochanteric fractures in the presence of knee arthroplasty: The role of intermediate length cephalomedullary nail. J Musculoskelet Surg Res. 2025;9:70-5. doi: 10.25259/JMSR_382_2024
Abstract
Objectives:
Despite the increasing popularity of intermediate-length cephalomedullary nails (ILCMNs), no studies reported their special role in situations involving distal femoral implants. This study highlights the use of ILCMNs in patients with low trochanteric fractures and total knee arthroplasty (TKA), where short or long nails were not utilized due to the fracture configuration or the presence of femoral implants, respectively.
Methods:
Out of 2621 cephalomedullary nails (CMNs) that were reviewed for this study, eight cases (8 females, mean age 77.8 years) developed low intertrochanteric fractures (AO/OTA 31 A2.3 or A3) in the presence of a stemmed (5 cases) or unstemmed (3 cases) TKA. All cases received 235 mm ILCMNs and four had an additional overlapping fixation with plates.
Results:
All the cases achieved radiographic bony union at a mean of 13.2 weeks postoperatively. After a mean follow-up of 52.3 months, none of the cases developed inter-prosthetic fractures or required revision.
Conclusion:
ILCMNs can be utilized as alternatives to long CMNs whenever knee arthroplasty is present.
Keywords
Cephalomedullary
Fracture
Hip
Intermediate length
Midlength
Nail
Proximal femoral
Trochanteric

INTRODUCTION
Intermediate-length (235–240 mm) cephalomedullary nails (ILCMNs) have been developed as alternatives to short and long cephalomedullary nails (CMNs) in trochanteric fractures to counterbalance their potential benefits and downsides. While providing more nail length distal to the locking screw compared to the short nails (SNs), intermediate nails employ the same distal locking screw location and targeting device as SNs. This facilitates the distal locking screw’s easy insertion and offers extra fit distal to the femur’s isthmus, which may be necessary for some fracture types that extend far distal to the lesser trochanter level.[1]
While the presence of long-stemmed total knee arthroplasty (TKA) makes the utilization of long femoral nails impossible, the presence of unstemmed TKA may potentially interfere with or be complicated after using long nails (LNs).[2] Despite several retrospective studies reporting on the outcomes of ILCMNs,[3,4] no reports highlighted their specific utility in cases with trochanteric fractures in the presence of TKA. This study aims to report our single institution experience and outcomes of the intermediate length, 235 mm CMNs for cases of low trochanteric fractures in the presence of stemmed or unstemmed TKA, where SNs were not used due to the fracture configuration, and LNs were not used due to the presence of TKA.
MATERIALS AND METHODS
After Institutional Review Board approval, we reviewed 2834 proximal femoral nailing cases performed at our institution between 2007 and July 2024, using our selection criteria to extract the relevant cases.
The study included cases with low trochanteric fractures (AO/OTA 31A2.2, A2.3 and A3), those with a preceding TKA and received intermediate-length, 235 or 240 mm proximal femoral nail. We excluded cases that did not complete a minimum of 6 weeks of radiographic follow-up.
A total of 9 cases (9 patients) met the inclusion criteria. One case was excluded due to incomplete follow-up, leaving 8 cases (8 patients) with complete data for inclusion in this study. Patient demographics, notes, and all pre-operative and post-operative radiographs were individually assessed to extract all relevant data. Time until radiographic healing, the last available clinical and radiographic follow-up dates, and any complications were recorded. In all cases, the 130° TFN-Advanced (DePuy Synthes Trauma) 235 mm (lock-short) nails were used based on the surgeon’s pre-operative or intraoperative decision for cases with trochanteric fractures in the presence of distal TKA (five stemmed, three unstemmed) as an alternative to short or long CMNs. In all cases, the fracture configuration made SNs an improper choice as per the surgeon’s decision (six cases had a reverse obliquity, AO/OTA 31A3 fracture type, and two had low intertrochanteric, AO/OTA 31 A2.3 fracture with broken lateral proximal femoral cortex).[5] As for the LN choice, the presence of a stemmed TKA renders the utilization of a LN not possible, while in the cases that had an unstemmed TKA, the surgeon decided to use ILCMN to avoid any potential interference with the TKA femoral component and any probable meddling with a future revision.
Clinical and radiographic assessment
Fracture classification, surgery duration, blood loss, and radiographic outcomes were recorded. Walking ability was determined according to whether the patient could walk independently, use an assistive device, or be wheelchair-bound.
Statistical analysis
Data analysis was performed using Microsoft Excel. Values were expressed as means, range, and standard deviation. The two-sample Welch’s t-test was used to compare the means and a value lower than 0.05 was considered statistically significant.
RESULTS
Patient demographics
A total of 8 cases in 8 females met the selection criteria and were reviewed in this study. Patients had a mean age of 77.8 years (62–87.6) at the time of surgery. The right side was involved in 7 cases. The mean patient height was 1.6 m (1.4–1.7 m), and the mean body mass index was 29.1 (19.1–42.7). Six patients had significant pre-operative medical comorbidities, and the mean American Society of Anesthesiologists score for all patients was 3 (2–4). Two patients died at a mean of 17.3 months postoperatively for causes unrelated to surgery. The remaining cases have a mean follow-up of 64 months (46.5–96). The average follow-up for all patients was 52.3 months.
Indications
Low trochanteric fractures that extend distal to the lesser trochanter (AO/OTA 31A2.3 and A3), in the presence of an ipsilateral TKA.
In this series, the utilization of ILCMN was decided preoperatively at the discretion of the surgeon after the assessment of the radiographs. In all cases in this series with low trochanteric fractures, ILCMNs rather than SN were utilized to achieve a distal diaphyseal fit, given the fracture extension distal to the lesser trochanter. ILCMN was also preferred to plate fixation due to its less invasive technique and also due to the fracture instability. In cases where there is stemmed TKA, LNs could not be used. In the cases where unstemmed TKA was present, utilization of ILCMN was decided to avoid any potential intraoperative or post-operative interference with the knee implant.
Surgical details
In 6 cases, a 235 × 10 mm nail was used; in the other 2 cases, a 235 × 11 mm was used. The average blood loss as per anesthesia records was 397 mL (25–1050). The mean estimated surgical duration was 150 min (72–225). Weight-bearing as tolerated with an assistive device has been started from the next day of surgery for all 8 cases.
Radiographic outcomes
No intraoperative complications were recorded. No nail jamming occurred, and all nails were successfully inserted below the end of the distal isthmus after appropriate reaming. Fracture union was noticed at a mean of 13.2 weeks (6.4–23.9) [Figures 1-3].
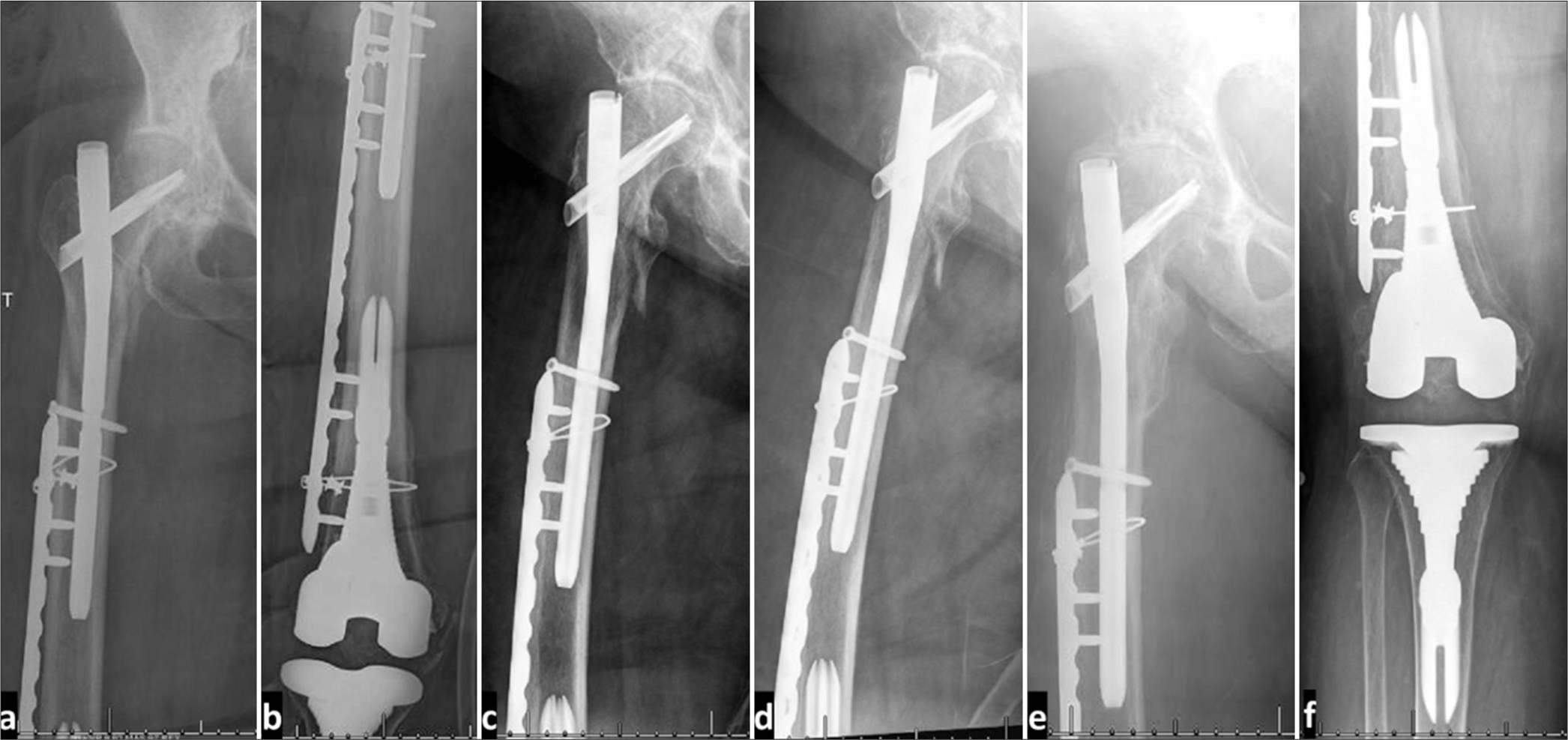
- (a and b) Immediate post-operative radiographs after open reduction and internal fixation using intermediate length proximal femoral nail with bridging plate for a 73-year-old female who sustained a low intertrochanteric fracture (AO/OTA 31A2.3) involving the proximal femoral lateral cortex, in the presence of a stemmed revision total knee arthroplasty that was inserted 1 month before. (c and d) 2-week follow-up radiographs showing maintained reduction. (e and f) 3-year follow-up radiographs showing fracture consolidation and maintained reduction.
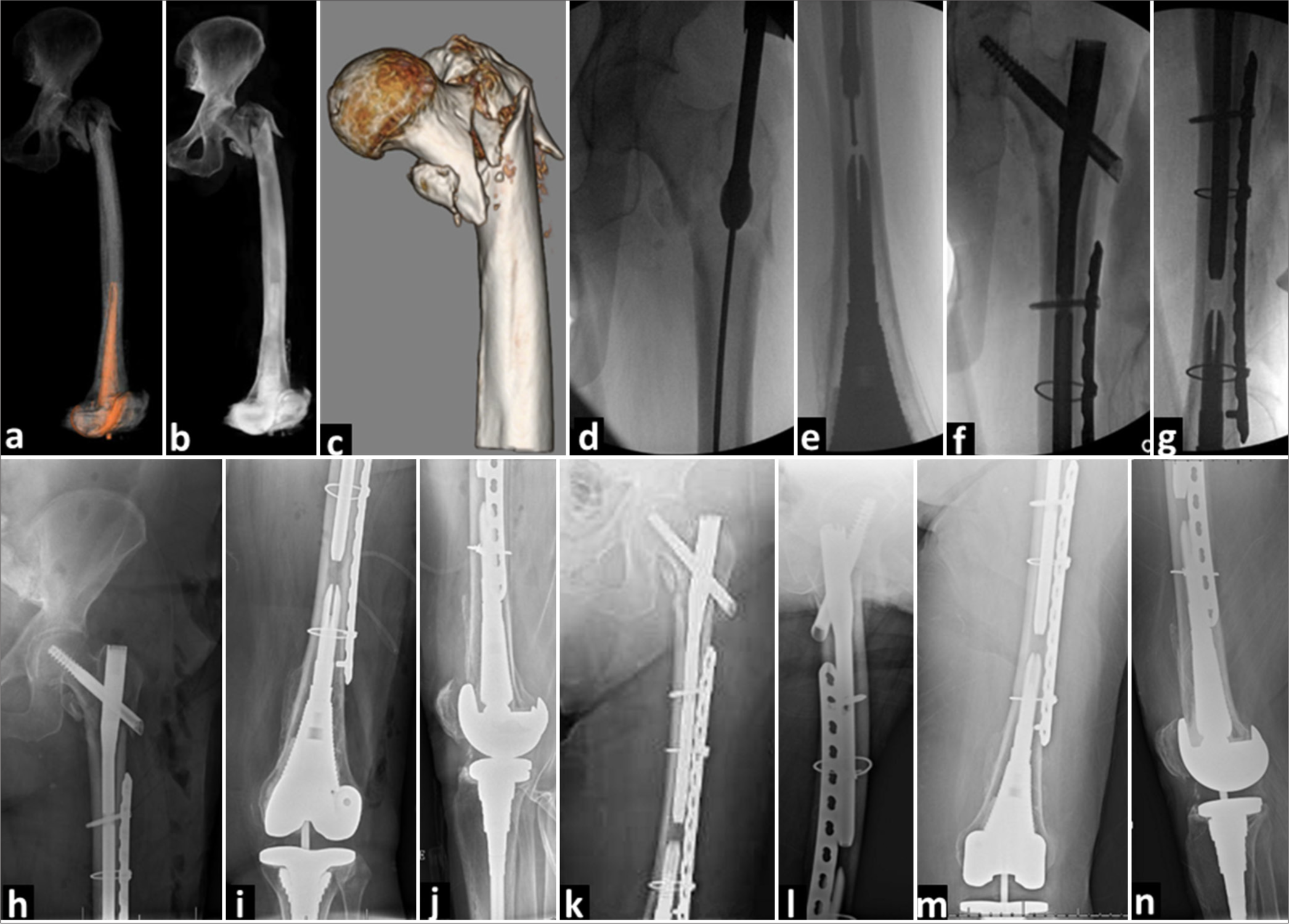
- (a-c) Plain radiographs of an 84-year-old male who sustained an intertrochanteric femoral fracture due to a fall. (d-g) Intraoperative C arm radiograph showing reduction with bridging fixation. The purpose of bridge plating is just to dissipate the stress riser at the end of the two opposing two intramedullary implants and not for fracture fixation. Consequently, the surgeon felt that plate fixation on either side of the nail could be sufficiently achieved with a single screw and cerclage wire. (h-j) Immediate post-operative radiographs. (k-n): 3-month follow-up anteroposterior and lateral radiograph showing fracture healing and stable fixation.
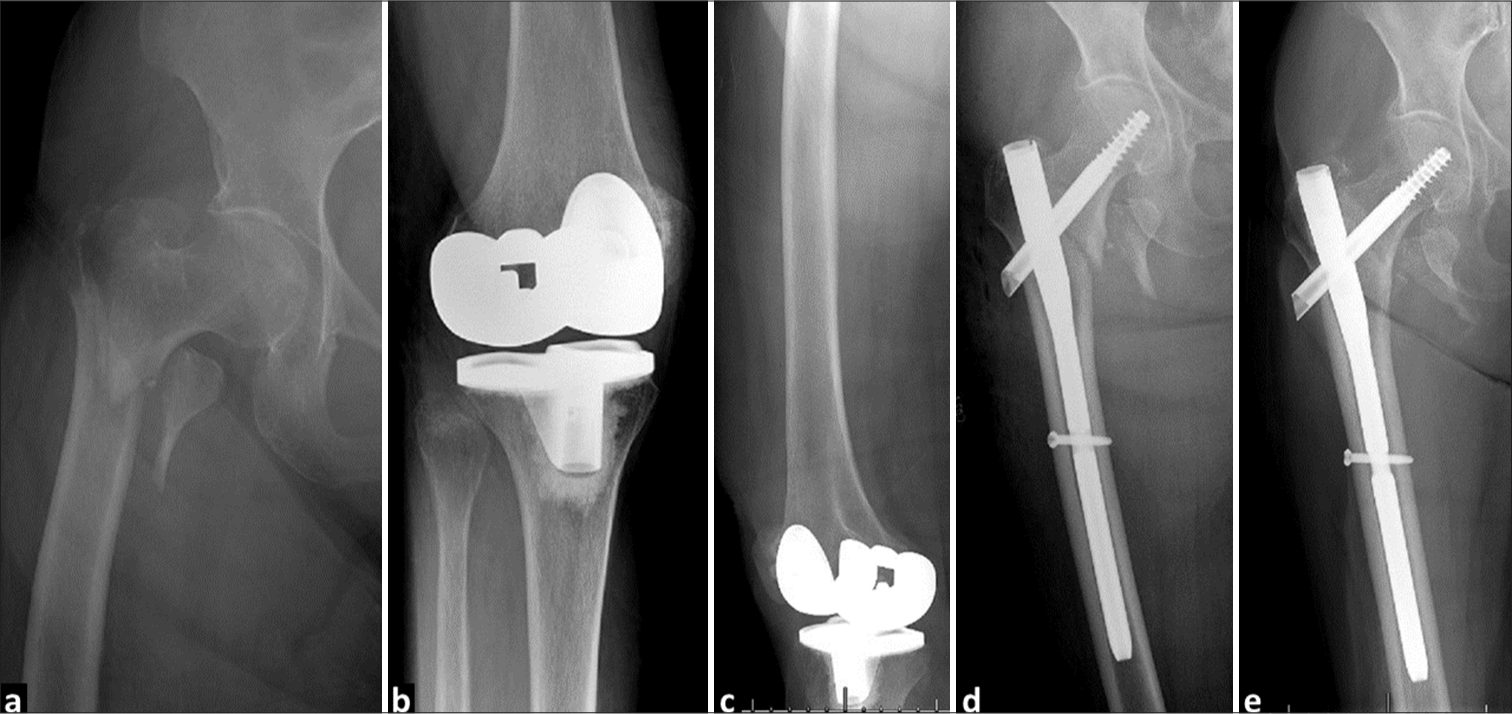
- (a) Plain hip radiograph of a 90-year-old female presented with AO/OTA 31A2.3 trochanteric fracture. (b and c) The patient also had a loose, malrotated total knee arthroplasty (TKA). (d) Immediate post-operative hip radiograph and (e) 8-week post-operative plain hip radiograph showing fracture healing after insertion of intermediate-length cephalomedullary nails (ILCMN). The surgeon opted for intermediate-length cephalomedullary nails rather than long cephalomedullary nails to avoid any potential interference with the TKA, which would potentially require revision.
Clinical outcomes
All patients were able to bear weight with assistive devices without significant pain or limping in the last related clinical follow-up visit, with a mean visual analog scale for pain of 0.7 (0–3) and a mean calculated Parker Mobility Index of 5.4 (3–6). None of the cases developed infections, hardware failure, periprosthetic fractures, thigh pain, or required revision at their last related clinical assessment.
Bridging with the distal implant
Five cases had stemmed TKA, and three had unstemmed TKA. For the cases that had stemmed TKA, four received bridge (overlapped) fixation, while one did not have bridging with the TKA stem. None of the cases with unstemmed TKA received overlapped fixation. Bridging was performed based on the surgeon’s discretion utilizing plates and screws with or without cerclage wires.[6] None of the 8 cases developed interprosthetic fracture or chronic pain at the nail end. The mean time until union in the bridged group was 13.1 ± 5.7 weeks versus 13.4 ± 8 weeks in the remaining cases. The difference was not found to be statistically significant (P = 0.95). None of the cases developed inter-prosthetic fractures after a mean follow-up of 55.3 and 49.3 months for those who received bridging and the other cases, respectively.
DISCUSSION
This is a retrospective series of 8 cases with trochanteric fractures in the presence of TKA that was surgically managed with the 235 mm ILCMNs. After a mean follow-up of 52.3 months, all the cases achieved full fracture healing and none had implant failure, infection, or required revision for any cause.
The choice of nail length in intertrochanteric fractures (AO/OTA 31 A1-3) is still debatable and dependent on several variables, such as the fracture’s nature, the bone’s quality, and the surgeon’s preference.[7] Due to their shorter surgery duration, relative ease of distal interlocking, less blood loss, and potentially lower costs, SNs (170–200 mm) are commonly utilized.[7,8] However, in many cases such as those with large femoral medullary canals, fractures with inadequate proximal lateral femoral cortex,[5] osteoporosis, pathologic fractures, fracture in patients with multiple falls,[9] and trochanteric fractures with subtrochanteric extension (AO/OTA 31 A2.3 and A3)[10] where SNs could not provide adequate fixation, LNs (300–480 mm) are more appropriate.
Conversely, potential drawbacks of LNs include lengthening the surgical procedure, necessitating more reaming, increased blood loss, raised costs, more difficult freehand distal locking insertion, and the potential mismatch between the nail and femoral shaft bow.[1]
ILCMNs have gained increasing popularity. They were intended to provide an equally simple surgical technique as SNs with more stability afforded by the distal femoral fit. Since their introduction, several studies[3,11] compared their outcomes to the more popular short or long CMNs. The findings of these studies suggest overall comparably good clinical and radiographic outcomes. Despite this, Enns et al.[4] reported a high incidence of proximal fixation cutout with ILCMNs, which may be attributed to the older nail designs or the use of helical blades rather than the nail length.
In this study, ILCMN has been utilized for a specific indication, where a pre-existing TKA limited the use of long CMNs and fracture configuration made SNs improper options. In these cases, ILCMN was found to be the most appropriate option due to the easier surgical technique and, more importantly, to avoid interfering with the distal implants.
The evidence behind the concept of bridging or overlapping fixation between two implants remains lacking. CampilloRecio et al.[12] recommended using prophylactic minimally invasive plate osteosynthesis between 2 intramedullary femoral implants (stemmed arthroplasty) to decrease the risk of secondary inter-prosthetic fracture given the increased stress risers and the decreased strength on such occasions. In our series, we have utilized bridging in 4 out of 5 cases that had a stemmed TKA, which was decided to be the standard of care in our hospital given the emerging, scarce evidence in this regard. The case that did not receive bridging was one of the first cases presented on this rare occasion.
Study limitations
This study has several limitations, being retrospective and non-comparative. Despite the rarity of this patient setting, the very small number of cases is also a major limitation that necessitates cautious interpretation of the outcomes and recommendations. Ideally, a prospective study comparing bridge plating versus non-bridging with a larger number of cases would be ideal to conclude stronger evidence regarding whether to add overlapped fixation to the construct, with its potential increased surgery time and blood loss. A study comparing intermediate-length nails with short and LNs would also be required to better conclude the potential values of the intermediate-length nails on this rare occasion. Despite these limitations, this study is just a trial to present the available evidence, considering the rarity of this trauma setting.
CONCLUSION
Considering the results of the current study, the intermediate length, 235 mm nails could provide adequate and safe fixation and good outcomes in cases of proximal femoral fractures in the presence of TKA. Bridging between the nail and a distal intramedullary implant may be utilized to protect the inter-prosthetic bone from the increased stresses and potentially decrease the potential fracture risk. Larger studies are required to provide stronger evidence.
RECOMMENDATIONS
In the presence of TKA, ILCMNs can be used to manage low intertrochanteric fractures.
AUTHORS’ CONTRIBUTIONS
ANM: Manuscript writing. ANM, HM, MS, and DSH: Conception, design, methodology, data analysis, and manuscript editing. SH, KS, and AN: Data collection and manuscript editing. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
ETHICAL APPROVAL
An institutional review board approval (Geisinger IRB 2019-0591, July 2019) has been obtained before commencing this retrospective study.
DECLARATION OF PATIENT CONSENT
Informed consent has been obtained for the surgical procedure and has been waived by the IRB, for publishing the de-identified clinical data devoid of protected health information, given the retrospective nature of the study.
USE OF ARTIFICIAL INTELLIGENCE (AI)-ASSISTED TECHNOLOGY FOR MANUSCRIPT PREPARATION
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Clinical outcome of mid-length proximal femoral nail for patients with trochanteric hip fractures: Preliminary investigation in a Japanese cohort of patients more than 70 years old. Geriatr Orthop Surg Rehabil. 2020;11:2151459320936444.
- [CrossRef] [PubMed] [Google Scholar]
- Failure of knee arthroplasty secondary to inadequate technique in cephalomedullary nailing of a subtrochanteric hip fracture. BMJ Case Rep. 2012;2012:bcr1220115430.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of short, intermediate, and long cephalomedullary nail length outcomes in elderly intertrochanteric femur fractures. J Am Acad Orthop Surg Glob Res Rev. 2022;6:e21.00322.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical outcomes of intermediate-length cephalomedullary nails for intertrochanteric femur fracture repair in older adults. Kans J Med. 2020;13:106-11.
- [CrossRef] [PubMed] [Google Scholar]
- Short cephalomedullary nail toggle: A closer examination. OTA Int. 2022;5:e185.
- [CrossRef] [PubMed] [Google Scholar]
- Adequate bone healing after supplementary fixation of periprosthetic total knee arthroplasty fractures using Luque cerclage wiring: A retrospective case series. Eur J Orthop Surg Traumatol. 2024;34:389-95.
- [CrossRef] [PubMed] [Google Scholar]
- Nail length in the management of intertrochanteric fracture of the femur. JAAOS J Am Acad Orthop Surg. 2016;24:e50-8.
- [CrossRef] [PubMed] [Google Scholar]
- A systematic review of short versus long intramedullary fixation in the management of pertrochanteric fractures. Trauma. 2018;20:161-8.
- [CrossRef] [Google Scholar]
- Short versus long cephalomedullary nails for the treatment of intertrochanteric hip fractures in patients older than 65 years. J Orthop Trauma. 2014;28:391-7.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical performance of short and long cephalomedullary nail constructs for stabilizing different levels of subtrochanteric fracture. Injury. 2022;53:323-33.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes after unstable pertrochanteric femur fracture: Intermediate versus long cephalomedullary nails. Eur J Trauma Emerg Surg. 2020;46:963-8.
- [CrossRef] [PubMed] [Google Scholar]
- Inter-implant fractures: An unmet medical need-a preventive approach proposal. Eur J Orthop Surg Traumatol. 2020;30:539-43.
- [CrossRef] [PubMed] [Google Scholar]




