
Translate this page into:
Prevalence of knee osteoarthritis in Saudi Arabia: A systematic literature review
*Corresponding author: Asim M. Makhdom, Department of Orthopedic Surgery, King Abdulaziz University, Jeddah, Saudi Arabia. asim.m.makhdom@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Makhdom AM, Bokhary OA. Prevalence of knee osteoarthritis in Saudi Arabia: A systematic literature review. J Musculoskelet Surg Res, 2023;7:235-40.
Abstract
Knee osteoarthritis (KOA) is the most affected joint and a leading cause of pain and functional limitation in the older population. Multiple studies have investigated the prevalence of KOA worldwide. However, research is very limited on this matter in Saudi Arabia. This review aimed to investigate the prevalence of KOA in Saudi Arabia and assess its prevalence. A standardized, systematic search strategy was conducted to identify observational studies that reported on the prevalence of KOA in Saudi Arabia. The search included published studies between January 2000 and April 2023. Six eligible studies were included for analysis. This included 1952 participants. The prevalence in these studies showed wide variability throughout the past two decades and was reported to range between 13% and 41%. Individuals above 40 had an average reported prevalence of 67.8% (16.2–71.4%). A significant association between KOA and an increased body mass index and female sex was found. Studies on KOA prevalence are limited in Saudi Arabia. Despite this, it is evident that the prevalence of KOA is high based on the available literature. Establishing a database registry, lifestyle modifications, and public awareness efforts may help reduce this disease’s impact on our population.
Keywords
Knee
Osteoarthritis
Prevalence
Saudi Arabia
Review

INTRODUCTION
In the category of musculoskeletal diseases, osteoarthritis (OA) is considered the most prevalent.[1] OA is a chronic disease that affects several body regions and is defined by cartilage degradation, arthritic bone hyperplasia, and subchondral bone sclerosis.[2] The knee is the most commonly affected joint and the leading cause of pain and functional limitation in the older population.[3] Prior joint injury, weight, sex, genetic factors, and anatomical variables linked to joint shape and alignment may all play a role in developing knee OA (KOA).[4] The most frequently utilized case definitions are symptomatic KOA, radiographic KOA, and self-reported KOA. KOA is considered symptomatic when both radiographic and joint symptoms associated with the disease are present.[5] Only pathologic signs of joint disease seen on radiographic images are considered in the radiographic definition.[6] In recent times, Saudi Arabia has witnessed a surge in the prevalence of obesity rates and alterations in lifestyle and dietary patterns.[7] Unfortunately, as a result, the general population has become more susceptible to KOA. Multiple studies reported the prevalence of KOA worldwide, including other Gulf countries, Europe, China, and the United States of America (USA).[8-10] However, research is very limited about this matter in Saudi Arabia. With a growing population and medical advancement, it is imperative to understand the burden of KOA and what challenges it poses to the health-care system. In some cases, early identification and management can reduce the accelerated progression. The primary objective of this review was to investigate the prevalence of KOA and its associations in Saudi Arabia.
MATERIALS AND METHODS
Preferred reporting items for systematic reviews and meta-analysis criteria were followed for conducting this review.
Search strategy
PubMed and Google Scholar were electronically searched by the two authors to identify studies published from January 2000 to April 2023. The search terms included “Knee osteoarthritis,” “prevalence or incidence or epidemiology,” and “Saudi Arabia.” The search phrases were combined in several ways to find relevant literature, and the search strategies were customized to suit each database. To find relevant studies, reference lists of eligible articles were also retrieved.
Inclusion criteria
The following criteria were included in the study:
Studies involving patients with KOA in Saudi Arabia
Studies recording data on the prevalence by sex, age, diagnostic criteria, and year
The type of study: random or cluster sampling.
Exclusion criteria
Studies conducted in special groups (e.g., pregnant women), published before the year 2000 and studies whose full texts were unavailable and could not be retrieved were excluded from the study.
Data extraction
Two reviewers independently assessed each study’s titles and abstracts against the inclusion and exclusion criteria. Articles that did not fit the inclusion requirements were removed. Further, analysis was performed in cases of doubt during any screening stage, and issues were addressed through consensus discussion. The prevalence was defined as the number of existing cases in a population during each study. Articles in the full text were assessed for eligibility. The remaining studies were included in the systematic review. One investigator extracted the data, which included (1) first author, (2) study year, (3) study design, (4) average age, (5) sex, and (6) diagnostic criteria of KOA.
RESULTS
The database search yielded 5150 papers; after removing duplicates, 5086 publications were reviewed by titles/ abstracts, and 5076 were eliminated. After that, seven of these papers were reviewed in full text, and one was excluded, yielding six included publications [Figure 1].
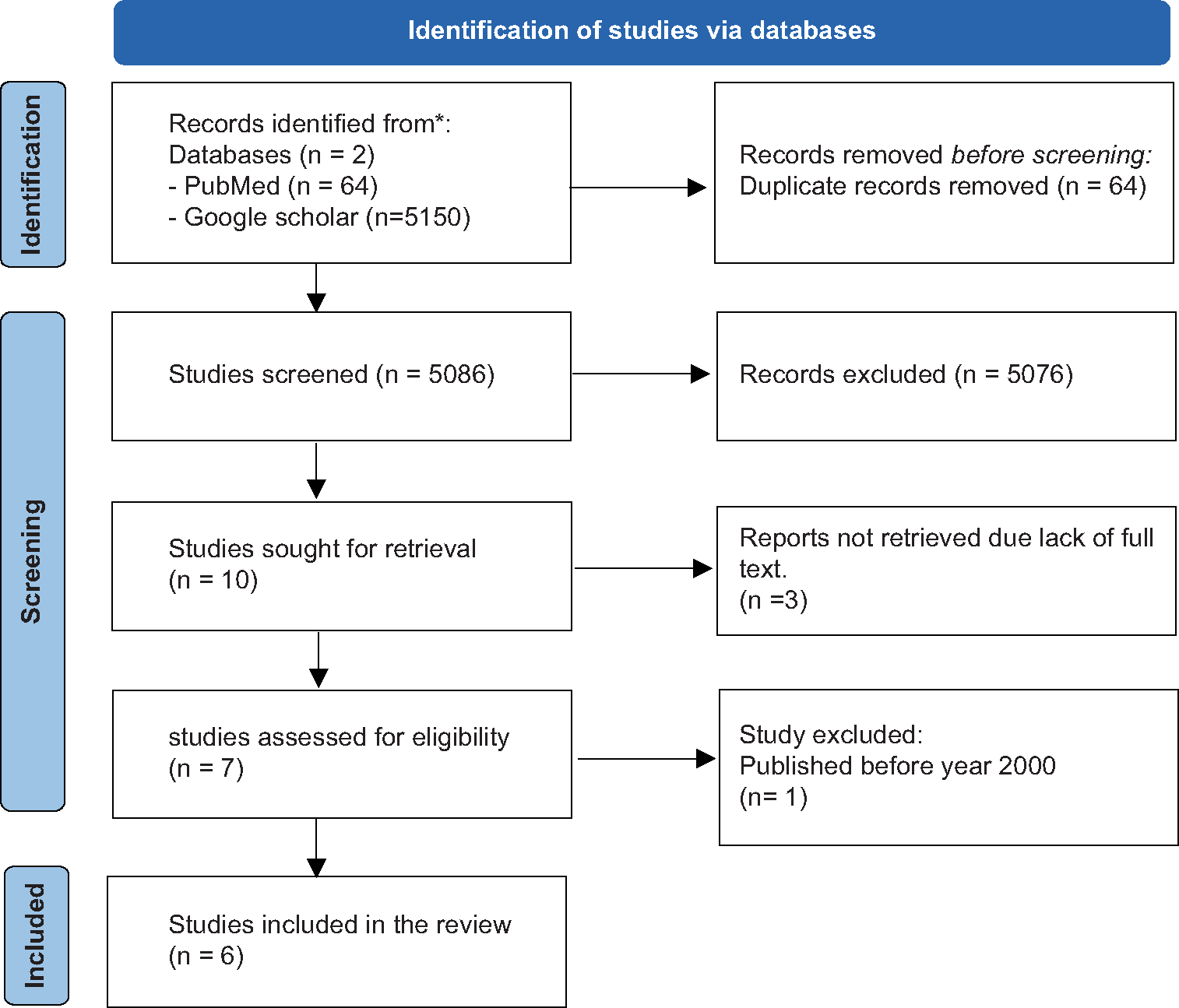
- Search and screening flow chart.
Characteristics of studies
A total of six papers were included in the review [Table 1]. The majority were cross-sectional (n = 5) studies, with one study conducted as a retrospective records review. In three studies, the diagnostic criteria for KOA were the American College of Rheumatology (ACR) criteria. Radiographic diagnoses were only used in two studies.
| Author | Year | Study design | Diagnostic criteria | Cases with OA | Region (City) | Mean age | Males (%) | Females (%) | Prevalence rate | Association with Sex | Association with *BMI |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Althomalia et al.[13] | 2023 | Cross-sectional study | *ACR | 425 | All | - | 56 (12.9) | 369 (20.25) | Overall 18.9% By Age 18–30: 6.8% 31–49: 20.2% 50<: 45.7% |
P<0.01 | <0.01 |
| Al-Arfaj and Al-Boukai.[14] |
2002 | Cross- sectional study | Radiographic | 170 | Central (Riyadh) | - | 89 (53.3) | 81 (60.9) | (56.67%) | - | - |
| AlKuwaity et al.[11] | 2018 | Cross- sectional study | - | 238 | Northern (Arar) |
70.4 (±9.3) | 115 (48.3) | 123 (51.7) | Overall 24.5% By Age >60: 24.7% >70: 32.3% >80: 21.7% |
P>0.05 | 0.041 |
| Thigah and Khan.[12] |
2020 | Cross- sectional study | *ACR | 200 | Western (Makkah) |
129 (64.5) | 71 (35.5) | Overall 41.5% |
P=0.889 | - | |
| Al-Arfaj et al.[16] | 2003 | Cross- sectional study | *ACR | 766 | Central (Alqaseem) |
- | - | - | Overall 13% By Age 16–25: 1.1% 26–35: 4.8% 36–45:16.2% 46–55: 30.8% 56–65: 47.8% 66–75: 60.6% 76–85: 58.8% >86: 42.9% |
- | - |
| Alrowaili.[15] | 2019 | Records review | Radiographic | 163 | Northern (Arar) | <40: 70 >40: 93 |
102 (31) | 61 (74.4) | Overall 39.75% By age <40: 25.6% 40–50: 60% 51–60: 79.2% 61–90: 71.4% |
<0.0001 |
Prevalence
The prevalence of KOA for each study is shown in [Table 1]. Individuals above 40 had an average reported prevalence of 67.8% (16.2–71.4%).[11-14] It was noted that the average prevalence between 2002 and 2011 was 34.83%, and between 2012 and 2021 was 35.25%. Overall, the prevalence in these studies showed wide variability in prevalence throughout the past two decades.
Sex discrepancies
When a bivariate analysis was done between KOA and sex, two studies showed a statistically significant relationship between females and KOA (P < 0.01).[13,15]
Body mass index (BMI)
Only two studies considered BMI as a variable and further analyzed it with KOA [Table 1]. The studies revealed a significant relationship between higher BMI and KOA (P < 0.01).[11,13]
DISCUSSION
The prevalence of KOA in Saudi Arabia appears to be high. Three studies reported a significantly higher prevalence in the older population, ranging from 41% to 79%.[12,15,16] In contrast, the prevalence of KOA in some neighboring countries in the Gulf region was reported to range between 6.5% and 94.2%.[17,18] This is considered higher than in some Asian and European countries. A systematic review and meta-analysis done in 2020 concluded a pooled prevalence of 14.6% in China,[9] while a study in Sweden revealed a prevalence of 24.5%. However, the prevalence of KOA in the USA was comparable to our findings and was found to be 37.4%.[8,10]
KOA is multifactorial, but one important modifiable variable is BMI. The global prevalence of obesity is increasing. A recent study in Saudi Arabia in 2021 showed that the national weighted prevalence of obesity (BMI ≥ 30) was 24.7%.[19] When compared to a study published in China, the prevalence was found to be 7.9%.[20] However, the Centers for Disease Control and Prevention reported the overall obesity prevalence in the USA as 36.5% in 2015.[21] The prevalence of obesity is significantly higher in Saudi Arabian and American populations compared to China, which may explain the high prevalence of KOA in both countries. One of the core drivers of the high prevalence of obesity in Saudi Arabia is the change in lifestyle and eating patterns in the past decades.[7] Saudi Arabia is second in the percentage of insufficient physical activity in adults and the top ten in processed meat consumption, according to the Global Obesity Observatory.[7] Furthermore, comorbidities such as hypertension, hypercholesterolemia, and diabetes play a significant role in obesity. A study in 2023 highlighted the increasing prevalence of these diseases in the Saudi population.[22] Awareness events about KOA and obesity as risk factors are required to help reduce such prevalence.
In two studies, KOA predominantly affected females (P < 0.01).[13,15] This finding was similar to a neighboring country (Qatar) where female predominance was also found.[17] Other Asian countries, such as Iran and China, concluded that females were the most prevalent in their analysis.[9,23] This is unsurprising as it is well known that females are more prone to presenting with KOA. It could be due to differences in knee anatomy, hormonal changes, and other individual factors such as genetic factors.[24]
We found wide variation in the prevalence of KOA over the past two decades. It is possible that differences in diagnostic criteria of KOA among the studies have contributed to such findings. Three studies used the ACR criteria for diagnosing KOA, which is based on the patient’s clinical symptoms to diagnose.[12,13,16] On the other hand, two studies opted to use the radiographic criteria.[14,15] The previous studies have discussed which criterion is preferable. It is believed that the radiographic definition has a propensity to exaggerate the incidence of OA. Some authors found that the incidence of KOA can be higher (twice as high) in the same participant when only the radiographic definition is utilized while ignoring the clinical symptoms.[25] This could explain the drastic change in prevalence between the two studies published in 2002 and 2003,[14,16] wherein the first study reported a 56.67% prevalence using the radiographic criteria. The study published the following year reported 13% when ACR criteria were implemented. We believe that future studies should focus on merging both clinical and radiographic criteria to diagnose KOA. Confident diagnosis can be made in adults with knee pain, functional limitation, and one or more typical examination findings (restricted movement, bony enlargement, and crepitus).[26] In addition, radiographs can serve as an objective tool for KOA pathophysiological findings.[27]
This review was limited by the scarcity of papers published about KOA prevalence in the country and the heterogeneity of diagnostic tools used to identify KOA. This may be due to our hospital’s lack of a database that reports diagnostic codes. The availability of such databases can be beneficial for researchers to investigate this topic. Therefore, this reported prevalence cannot be extrapolated to all regions in Saudi Arabia. However, our review showed a pattern of potential increased prevalence throughout the past two decades, which is critical for the health-care system, physicians, and researchers. Second, the study provided a brief review of the state of the disease in Saudi Arabia. It opens the door for future researchers to investigate this disease’s prevalence more comprehensively and methodologically.
CONCLUSION
Studies on KOA prevalence are limited in Saudi Arabia. Despite this, a high prevalence of KOA was found, with female sex and high BMI being significant associations. Public awareness events about the risk of obesity and lifestyle modifications are required. A nationwide study and establishing a data registry for patients will be extremely helpful in evaluating the burden of this disease.
AUTHOR CONTRIBUTION
AMM conceived and designed the study, AMM and OAB conducted research, provided research materials, and collected and organized the data. AMM and OAB analyzed and interpreted data. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
ETHICAL APPROVAL
An ethics statement is not applicable, because this study is based exclusively on published literature.
USE OF ARTIFICIAL INTELLIGENCE (AI)-ASSISTED TECHNOLOGY FOR MANUSCRIPT PREPARATION
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
DECLARATION OF PATIENT CONSENT
Patients' consent is not applicable, because this study is based exclusively on published literature.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Prevalence of self reported musculoskeletal diseases is high. Ann Rheum Dis. 2003;62:644-50.
- [CrossRef] [PubMed] [Google Scholar]
- Knee pain and osteoarthritis in older adults: A review of community burden and current use of primary health care. Ann Rheum Dis. 2001;60:91-7.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of exercise on articular cartilage in people at risk of, or with established, knee osteoarthritis: A systematic review of randomised controlled trials. Br J Sports Med. 2019;53:940-7.
- [CrossRef] [PubMed] [Google Scholar]
- Ageing and the pathogenesis of osteoarthritis. Nat Rev Rheumatol. 2016;12:412-20.
- [CrossRef] [PubMed] [Google Scholar]
- Descriptive epidemiology of osteoarthritis in British Columbia, Canada. J Rheumatol. 2007;34:386-93.
- [Google Scholar]
- Prevalence and pattern of radiographic hand osteoarthritis and association with pain and disability (the Rotterdam study) Ann Rheum Dis. 2005;64:682-7.
- [CrossRef] [PubMed] [Google Scholar]
- Saudi Arabia. Available from: https://data.worldobesity.org/country/saudi-arabia-186 [Last accessed on 2023 Jul 13]
- [Google Scholar]
- Prevalence of knee pain and knee OA in southern Sweden and the proportion that seeks medical care. Rheumatology (Oxford). 2015;54:827-35.
- [CrossRef] [PubMed] [Google Scholar]
- The prevalence of symptomatic knee osteoarthritis in relation to age, sex, area, region, and body mass index in China: A systematic review and meta-analysis. Front Med (Lausanne). 2020;7:304.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of knee osteoarthritis in the United States: Arthritis data from the third national health and nutrition examination survey 1991-94. J Rheumatol. 2006;33:2271-9.
- [Google Scholar]
- Prevalence and determinant factors of osteoarthritis of the knee joint among elderly in Arar, KSA. Egypt J Hosp Med. 2018;72:5173-7.
- [CrossRef] [Google Scholar]
- Prevalence of knee osteoarthritis among adult patients attending Al-Iskan primary health care center, Makkah, Saudi Arabia. Ann Clin Anal Med. 2018;9:272-8.
- [Google Scholar]
- Prevalence of symptomatic knee osteoarthritis in Saudi Arabia and associated modifiable and non-modifiable risk factors: A population-based cross-sectional study. Healthcare (Basel). 2023;11:728.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of radiographic knee osteoarthritis in Saudi Arabia. Clin Rheumatol. 2002;21:142-5.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance evaluation of knee osteoarthritis among the Saudi Population. Pak J Med Sci. 2019;35:1575-81.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of musculoskeletal complaints and diseases in Qatar: A cross-sectional study. Qatar Med J. 2020;2020:29.
- [CrossRef] [PubMed] [Google Scholar]
- Characteristics of osteoarthritis among Kuwaitis: A hospital-based study. Clin Rheumatol. 1998;17:210-13.
- [CrossRef] [PubMed] [Google Scholar]
- Obesity in Saudi Arabia in 2020: Prevalence, distribution, and its current association with various health conditions. Healthcare (Basel). 2021;9:311.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of overweight, obesity, abdominal obesity and obesity-related risk factors in southern China. PLoS One. 2017;12:e0183934.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of obesity among adults and youth: United States, 2011-2014. NCHS Data Brief. 2015;219:1-8.
- [CrossRef] [PubMed] [Google Scholar]
- National and regional rates of chronic diseases and all-cause mortality in Saudi Arabia-analysis of the 2018 household health survey data. Int J Environ Res Public Health. 2023;20:5254.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of musculoskeletal disorders in Azar cohort population in Northwest of Iran. Rheumatol Int. 2017;37:495-502.
- [CrossRef] [PubMed] [Google Scholar]
- Knee osteoarthritis in women. Curr Rev Musculoskelet Med. 2013;6:182-7.
- [CrossRef] [PubMed] [Google Scholar]
- The incidence and natural history of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study. Arthritis Rheum. 1995;38:1500-5.
- [CrossRef] [PubMed] [Google Scholar]
- EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann Rheum Dis. 2010;69:483-9.
- [CrossRef] [PubMed] [Google Scholar]
- Osteoarthritis of finger joints in Finns aged 30 or over: Prevalence, determinants, and association with mortality. Ann Rheum Dis. 2003;62:151-8.
- [CrossRef] [PubMed] [Google Scholar]




