Translate this page into:
Prevalence of neck–shoulder pain and low back pain among high school students in Riyadh, Saudi Arabia
2 Department of Orthopaedics, King Saud University, College of Medicine, Riyadh, Saudi Arabia
Corresponding Author:
Rawaf K Al Rawaf
Hittin, Riyadh
Saudi Arabia
rawaf.k.r@gmail.com
| How to cite this article: Al Rawaf RK, Zamzam MM, Al Rehaili OA, Al Shihri AF, Abunayan MS, Al Dhibaib AA, Al Jafar AF, Al Barakah AF. Prevalence of neck–shoulder pain and low back pain among high school students in Riyadh, Saudi Arabia. J Musculoskelet Surg Res 2019;3:279-285 |
Abstract
Objectives: Neck–shoulder pain (NSP) and low back pain (LBP) can interfere with a normal function that affect work productivity, daily activity, and comfortable sleeping. On the long term, it could cause musculoskeletal disability. The prevalence of this pain is unknown among adolescents in Riyadh. The purpose of the study is to measure the prevalence of NSP and LBP among high schools' students in Riyadh and to pinpoint the associated possible causes responsible for their occurrence. Methods: This is a quantitative, observational cross-sectional study done in Riyadh. We have selected five high schools, from different regions of the city. We have performed the study using a self-administered questionnaire administered to 596 adolescent students at the five selected high schools in Riyadh. Results: A total of 563 (56.0% of males and 44.0% of females) participants completed the questionnaire. Around half of the samples (49.7%) reported to have both NSP and LBP, and 18.1% reported that they have experienced neither NSP nor LBP. NSP was reported by 69.4% of participants and was significantly associated with female gender and mood change and abdominal sleeping position. LBP, on the other hand, was reported by 62.2% of participants and was significantly associated with female gender and mood change. Conclusions: NSP and LBP are common problems among high school students in Riyadh. Being female, having mood changes, and abdominal sleeping position are risk factors.
Introduction
The prevalence of neck–shoulder pain (NSP) and low back pain (LBP) among adolescents has increased in the last three decades. One of the contributing factors for that increase is the use of computer and mobile phones for prolonged period.[1] Neck and shoulder are considered the most commonly affected musculoskeletal locations for nontraumatic pain in adolescents in both genders, while the lower back is the third common location.[2]
Neck pain has an annual prevalence rate of >30%, so it is considered the fourth leading cause of disability. Acute neck pain usually resolves with or without treatment, but almost 50% of patients will continue to suffer a recurrence of pain to some degree.[3]
The incidence of NSP in the young population is high, and the causes are multifactorial.[4] In girls, an increased prevalence of neck pain is related to sedentary activities such as television watching and reading books. In boys, high prevalence of NSP is associated with prolonged sitting and playing or working with a computer.[5] Around 7.6% of the adult population have neck pain at least once at some time in their life.[6]
On different studies, female gender, older age, hyperactivity, competitive sports, reduced life quality, and emotional symptoms are considered to be the most common factors associated with LBP.[7],[8],[9],[10]
LBP has a similar prevalence to that of neck pain of 7.6%. Although many patients experience acute self-limited LBP without the need to visit a physician, having LBP at working life is more common on people who suffered LBP earlier at adolescent hood.[11],[12],[13],[14]
The goal of the study was to measure the prevalence of NSP and LBP among high school students and the associated risk factors, in Riyadh, and to identify the associated factors responsible for their occurrence.
Materials and Methods
A quantitative cross-sectional study was performed to measure the prevalence of NSP and LBP among high school adolescents. Approval was obtained from the Institutional Review Board at the Medical College, King Saud University. The study was performed in Riyadh, the capital city of Saudi Arabia. The study was conducted at five high schools chosen randomly distributed in different regions of the city; three of them were male schools while two were female schools. Three schools were public schools while two were private. Our target was to obtain answers for the questionnaire from more than 500 students with at least 200 from each gender, and this number would allow a reliable statistical analysis. The study included 596 students. Any student who is younger than 14 or older than 19 years was excluded. We developed an Arabic questionnaire with a guide from previous similar studies,[1],[15] and then, this questionnaire was reviewed and readjusted by the spinal unit in our institute. The questionnaire was distributed to the students during the break time, and the instructions and the meaning of the terms in the questionnaire (physical activity, mood changes, and others) were explained to the students before answering. Each student had to sign a consent and was informed that he/she had the right to withdraw at any time without completing the questionnaire. Participants' secrecy was assured by giving each participant a code number, so demographic data of each participant did not appear belonging to the participant but belonging to a number. No incentives or rewards were given to any participant.
The questionnaire was tested on 10 students to ensure the simplicity and clarity of information and define the time needed to complete the questionnaire. Data of these 10 students were not included in the current study. The final questionnaire contained 30 questions in four pages divided into three sections. The first was the demographic characteristics of the participant, in addition to the risk factors, which included physical activity, time spent on computers and smartphones, medical illnesses, mood changes, and sleep position habit. The second section was verifying if the participant had NSP or not. For those who answered “Yes” there were six questions about the details of their pain. These details include onset, timing and severity of the pain, cause responsible for their pain, and specific time or situation for feeling the pain. They also include the effect of pain on their daily activities, walking, sleeping, mood and studying performance. In addition, there were four questions regarding visiting a doctor, ordering any laboratory or radiological tests, prescribing any medication, and finally, if they know the diagnosis of their problem. Participants were instructed to skip the second section and go directly to the third section if the answer was “No.” The third section was about LBP and had the same 10 questions for NSP. In case the participant answered “No,” he was asked to skip the third section and he will be done with the questionnaire.
Demographics and baseline characteristics were recorded. Descriptive results regarding categorical variables were given as percentages, while continuous variables were presented as mean and their corresponding standard deviation. Categorical variables were compared using the Chi-squared test. Subsequently, a post hoc analysis using the adjusted residual values was done to interpret a deeper inference on this strong association evidence. Whereas, continuous variables were compared using a paired t-test or Student's t-test, as appropriate.
The associations between different factors and the incidence of neck pain or back pain were analyzed using univariate and multivariate logistic regression models. Univariate odds ratios (ORs) and 95% confidence intervals (CI) were used to report risk for categorical variables. This was followed by entering back each excluded factor to determine any improved value to the model. Such a factor was retained in the final model if there was a significant improvement in overall value or if it confounded other existing factors. Estimates of the logistic regression models were reported to measure the strength of association, summarized as the exponentiated coefficient, and interpreted as ORs and their 95% CI. Interaction of factors in the multivariate model was tested for significance using the likelihood ratio test, but no interaction term contributed to the final models. The goodness of fit of the final model was assessed using the Hosmer–Lemeshow test.
For the missing survey data, whether total nonresponse or partial response, listwise deletion method was used. As a result, patients with missing values on a certain variable were deleted from the analysis of that specific variable.[16]
SPSS software version 23 (SPSS Inc., Chicago, Illinois, USA) was used for data entry and analysis. All analyses were carried out at a significance level of 0.05.
Results
Out of 596 students, a total of 563 participants (94.5%) completed the survey. There were 315 (56%) males and 248 (44%) females. The mean age of all participants was 16.59 years (SD ± 0.94). As mentioned in our methods, any participant who failed to answer a question was excluded from the analysis of that specific question. [Table - 1] illustrates the demographics and baseline characteristics of the study sample.
![[Table - 1]](#tbl_SaudiOrthopJ_2019_3_3_279_262815_t6.jpg){kind=link}

After conducting the Chi-square test, NSP showed a significant association with gender, mood change, and sleeping position with P < 0.001. On the other hand, LBP was significantly associated with gender and mood change with P < 0.001 [Table - 2] and [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4], [Figure - 5].
![[Table - 2]](#tbl_SaudiOrthopJ_2019_3_3_279_262815_t7.jpg){kind=link}
![[Figure - 1]](#fig_SaudiOrthopJ_2019_3_3_279_262815_f1.jpg){kind=link}
![[Figure - 2]](#fig_SaudiOrthopJ_2019_3_3_279_262815_f2.jpg){kind=link}
![[Figure - 3]](#fig_SaudiOrthopJ_2019_3_3_279_262815_f3.jpg){kind=link}
![[Figure - 4]](#fig_SaudiOrthopJ_2019_3_3_279_262815_f4.jpg){kind=link}
![[Figure - 5]](#fig_SaudiOrthopJ_2019_3_3_279_262815_f5.jpg){kind=link}

 |
| Figure 1: A clustered bar chart illustrating a significant association between gender and neck–shoulder pain with P < 0.001. Data labels represent frequencies corresponding to that specific category |
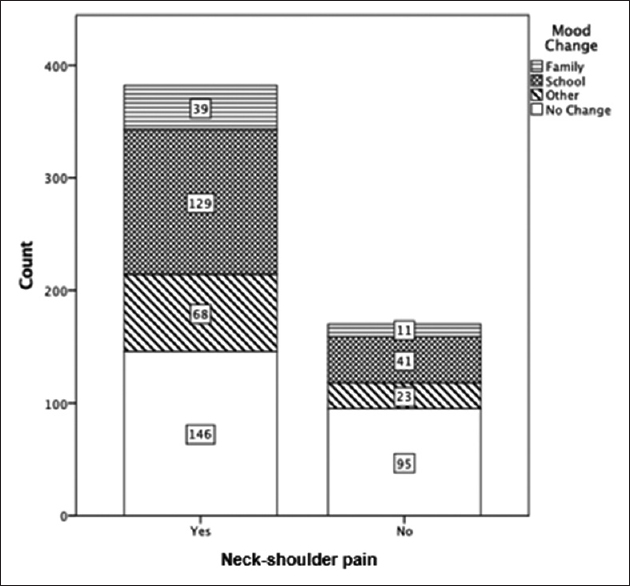 |
| Figure 2: A clustered bar chart illustrating a significant association between mood change and neck–shoulder pain with P < 0.001. Data labels represent frequencies corresponding to that specific category |
 |
| Figure 3: A clustered bar chart illustrating a significant association between sleeping position and neck–shoulder pain with P = 0.032. Data labels represent frequencies corresponding to that specific category |
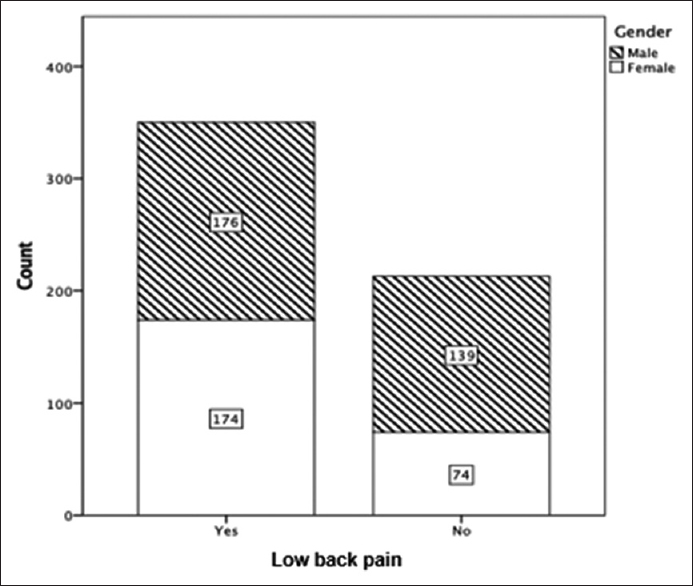 |
| Figure 4: A clustered bar chart illustrating a significant association between gender and low back pain with P < 0.001. Data labels represent frequencies corresponding to that specific category |
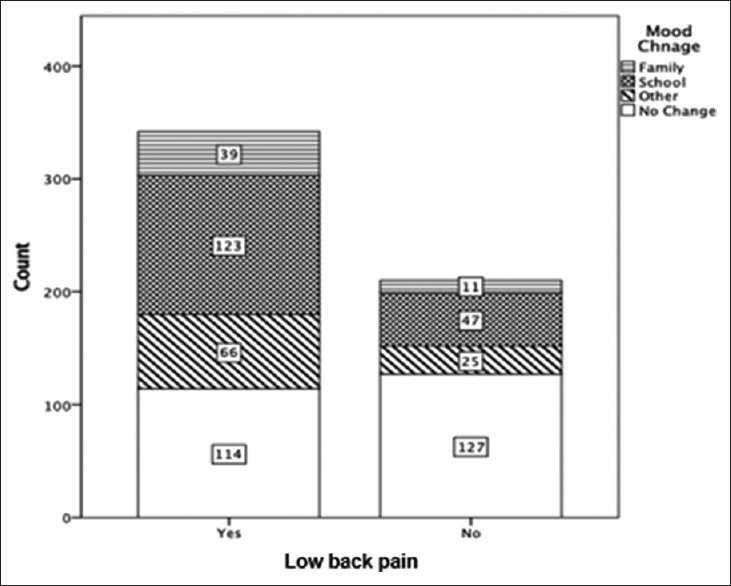 |
| Figure 5: A clustered bar chart illustrating a significant association between mood change and low back pain with P < 0.001. Data labels represent frequencies corresponding to that specific category |
[Table - 3] shows a cross tabulation, from which a Chi-square test was conducted to measure the level of association between NSP and LBP. From a total of 563 participants, who answered NSP and LBP questions, 280 (49.7%) reported to have both NSP and LBP and 102 (18.1%) reported that they have experienced neither NSP nor LBP. Using the Chi-square test, we found that this association was statistically significant, in which participants with NSP are most likely to have LBP as well (P < 0.001). [Table - 4] illustrates the responses of frequencies and percentages for the survey questions.
![[Table - 3]](#tbl_SaudiOrthopJ_2019_3_3_279_262815_t8.jpg){kind=link}
![[Table - 4]](#tbl_SaudiOrthopJ_2019_3_3_279_262815_t9.jpg){kind=link}


Males had lower odds reporting NSP compared to females (OR: 0.426, CI: 0.29–0.63, P = 0.001). Participants who sleep on the abdomen reported higher odds of NSP compared to participants who sleep on their back or on their side (OR: 2.97, CI: 2.74–4.41, P = 0.001) [Table - 5].
![[Table - 5]](#tbl_SaudiOrthopJ_2019_3_3_279_262815_t10.jpg){kind=link}

Males had lower odds reporting LBP compared to females (OR: 0.528, CI: 0.370–0.752, P = 0.001). Participants who experienced mood change due to school or family factor had higher odds of reporting LBP compared to participants who do not have mood changes with OR of 4.83 (CI: 2.09–9.17) and 2.98 (CI: 1.95–4.55), respectively [Table - 6].
![[Table - 6]](#tbl_SaudiOrthopJ_2019_3_3_279_262815_t11.jpg){kind=link}

It was important to capture the participants' insight from a quality of life perspective. When asked, 274 (71.9%) participants who reported NSP and 237 (75.2%) participants who reported LBP did agree that the associated pain influenced their daily activity significantly. In-depth analysis regarding the reasons behind these statements may be beyond the scope of this paper. However, further qualitative analysis through focus groups done with patients will provide deeper understanding of the underlying facts that could help facilitate health care decision making.
Discussion
Multiple studies stated that LBP is one of the most common causes of hospital visits and is considered to be the primary cause of activity restrictions and work absences. On the other hand, NSP is known to be a common complaint in adolescents and sometimes a disabling factor.[17],[18],[19]
This study found that the prevalence of NSP and LBP among adolescents is 69.4% and 62.2%, respectively, which is significantly higher than other studies conducted in multiple regions around the world among adolescents.[10],[20],[21],[22],[23],[24] We did not identify any specific reason for high school students in Saudi Arabia to explain this high prevalence. As shown in the present study, participants who experienced mood changes due to school or family had a significantly increased prevalence of LBP.
Males have experienced NSP and LBP significantly less than females in our study. This observation agrees with previous studies, which showed some gender distribution.[1],[10],[15],[20],[23],[24],[25],[26],[27],[28] However, some other studies reported that males are more likely to have LBP or there is no significant difference between genders.[21],[29] According to our results and the results of previous authors, there is a difference between males and females in having NSP or LBP, which could be related to different pain thresholds between genders and different hormonal changes during puberty and sedentary lifestyle.[23],[30],[31]
The present study identified that mood disturbance is associated with LBP, which agrees with the findings in other previous studies.[24],[32],[33] The authors who were investigating older age group in the Gulf region had reported a significant association of depression with LBP.[34],[35],[36] Furthermore, in agreement with some previous authors,[24],[25],[37] our study showed a significant association between mood change and NSP in adolescents.
A significant relationship between the position of sleep and NSP was noticed in the current study, which is not the case for LBP. Other studies found that there is a significant relationship between sleep period or sleep difficulties and NSP.[4],[19] Furthermore, some authors reported a significant relationship between the uncomfortable bed or fatigue symptoms and LBP,[4],[29] while Lusa et al.[38] found a strong association between disturbance of sleep and LBP among Finnish firefighters.
According to our results, there is a significant relation between NSP and LBP, which is consistent with the findings of Vikat et al.[19] Hakala et al., in their study,[39] showed a similar prevalence of NSP and LBP but with no significant association.
Surprisingly, our study did not show any significant association between using computers and NSP or LBP. We postulate the reason for this observation to the fact of book-based teaching among Saudi students. Although some studies had the same result,[15],[24] other studies have shown a significant risk in using computers to have NSP or LBP.[1],[40] Hakala et al. showed that using a computer >2–3 h is related to NSP and >5 h is related to LBP.[1] Silva et al. showed a similar result to Hakala et al. regarding LBP.[1],[41] However, Shan et al. showed an association between NSP and the use of computers.[20] AlShayhan and Saadeddin in their study among health sciences students using computers >10 h found a significant association with LBP.[29] Age differences could be a contributing factor for the differences while comparing with our results.
Our results showed no significant association between smartphone use and NSP or LBP, which agree with the results of Hakala et al.;[1] however, Silva et al. found that the use of mobile phones for >5 h was associated with LBP.[41]
Surprisingly, our results showed that physical activity had no significant association with NSP or LBP and that corresponds with the results of Diepenmaat et al.[24] Nevertheless, many studies reported a significant association.[4],[5],[15],[17]
In the present study, the prevalence of students visiting doctors was 8.5% and 9.5% for NSP and LBP, respectively, which is close to a study conducted in Portugal, which showed that 13.2% of students complaining of LBP visited doctors.[10] However, the figure is very low in comparison with another study, which reported that visiting a practitioner for NSP reached 47.1%.[25]
This study showed that participants with NSP or LBP reported a limitation of daily activity, similarly to the results of Hoftune et al. and Silva et al., who share the same age group with our study.[2],[21] Another study also reported limitation of activity in 34% of their participants with back pain, but the study was concerning a younger age group of 11–14 years.[40] Furthermore, 82% of participants in Skaggs et al. believed that heavy backpacks are the cause of musculoskeletal pain.[40] Silva et al. reported that in 70% of students with back pain, their pain is triggered or exaggerated by school seats.[41] In our study, 68.3% and 64.3% of the participants declared that wrong sitting posture is the main cause for NSP and LBP, respectively.
The main limitation of our study is the inability to determine the causality. Being a cross-sectional study, we could determine the association only. Another limitation is that we did not assess the body weight, height, and BMI of the participants. Moreover, our results could not be applied to adolescent, as we limited the age of the participants between 14 and 19 years of age.
Conclusions
NSP and LBP are common problems among high school students in Riyadh. Being female, having mood change, and abdominal sleeping position are risk factors.
Recommendations
Further study with expanding the age range to include all adolescents is recommended, which also should have more questions to identify the cause, the degree of the pain, limitations, and disabilities caused by LBP and NSP.
Ethical consideration statement
Ethical approval was obtained from the Institutional Review Board at the Medical College, King Saud University.
Acknowledgments
The authors are greatly thankful for the help of Monira K. Al Hasan, Ebtesam S. Al Mutairi, Rawan A. Al Rehaili, and Laila M. Al Sabbagh for their contributions in data acquisition.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Authors' contributions
RKR, MMZ, OAR, and AFS conceived and designed the study, conducted research, provided research materials, and collected and organized data. AAD and MSA analyzed and interpreted data. AFJ and AFB wrote the initial and final draft of the article and provided logistic support. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
| 1. | Hakala PT, Rimpelä AH, Saarni LA, Salminen JJ. Frequent computer-related activities increase the risk of neck-shoulder and low back pain in adolescents. Eur J Public Health 2006;16:536-41. [Google Scholar] |
| 2. | Hoftun GB, Romundstad PR, Zwart JA, Rygg M. Chronic idiopathic pain in adolescence – High prevalence and disability: The young HUNT study 2008. Pain 2011;152:2259-66. [Google Scholar] |
| 3. | Murray CJ, Atkinson C, Bhalla K, Birbeck G, Burstein R, Chou D, et al. The state of US health, 1990-2010: Burden of diseases, injuries, and risk factors. JAMA 2013;310:591-608. [Google Scholar] |
| 4. | Siivola SM, Levoska S, Latvala K, Hoskio E, Vanharanta H, Keinänen-Kiukaanniemi S. Predictive factors for neck and shoulder pain: A longitudinal study in young adults. Spine (Phila Pa 1976) 2004;29:1662-9. [Google Scholar] |
| 5. | Auvinen J, Tammelin T, Taimela S, Zitting P, Karppinen J. Neck and shoulder pains in relation to physical activity and sedentary activities in adolescence. Spine (Phila Pa 1976) 2007;32:1038-44. [Google Scholar] |
| 6. | Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur Spine J 2006;15:834-48. [Google Scholar] |
| 7. | Watson KD, Papageorgiou AC, Jones GT, Taylor S, Symmons DP, Silman AJ, et al. Low back pain in schoolchildren: The role of mechanical and psychosocial factors. Arch Dis Child 2003;88:12-7. [Google Scholar] |
| 8. | Lemos AT, Santos FR, Moreira RB, Machado DT, Braga FC, Gaya AC. Low back pain and associated factors in children and adolescents in a private school in Southern Brazil. Cad Saude Publica 2013;29:2177-85. [Google Scholar] |
| 9. | Harreby MS, Nygaard B, Jessen TT, Larsen E, Storr-Paulsen A, Lindahl A, et al. Risk factors for low back pain among 1.389 pupils in the 8th and 9th grade. An epidemiologic study. Ugeskr Laeger 2001;163:282-6. [Google Scholar] |
| 10. | Minghelli B, Oliveira R, Nunes C. Non-specific low back pain in adolescents from the South of Portugal: Prevalence and associated factors. J Orthop Sci 2014;19:883-92. [Google Scholar] |
| 11. | Hanvold TN, Veiersted KB, Waersted M. A prospective study of neck, shoulder, and upper back pain among technical school students entering working life. J Adolesc Health 2010;46:488-94. [Google Scholar] |
| 12. | Brattberg G. Do pain problems in young school children persist into early adulthood? A 13-year follow-up. Eur J Pain 2004;8:187-99. [Google Scholar] |
| 13. | Carey TS, Evans AT, Hadler NM, Lieberman G, Kalsbeek WD, Jackman AM, et al. Acute severe low back pain. A population-based study of prevalence and care-seeking. Spine (Phila Pa 1976) 1996;21:339-44. [Google Scholar] |
| 14. | Pellisé F, Balagué F, Rajmil L, Cedraschi C, Aguirre M, Fontecha CG, et al. Prevalence of low back pain and its effect on health-related quality of life in adolescents. Arch Pediatr Adolesc Med 2009;163:65-71. [Google Scholar] |
| 15. | Shan Z, Deng G, Li J, Li Y, Zhang Y, Zhao Q. Correlational analysis of neck/shoulder pain and low back pain with the use of digital products, physical activity and psychological status among adolescents in Shanghai. PLoS One 2013;8:e78109. [Google Scholar] |
| 16. | Troxel AB, Fairclough DL, Curran D, Hahn EA. Statistical analysis of quality of life with missing data in cancer clinical trials. Stat Med 1998;17:653-66. [Google Scholar] |
| 17. | Perry MC, Straker LM, O'Sullivan PB, Smith AJ, Hands B. Fitness, motor competence and body composition as correlates of adolescent neck/shoulder pain: An exploratory cross-sectional study. BMC Public Health 2008;8:290. [Google Scholar] |
| 18. | Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol 2010;24:783-92. [Google Scholar] |
| 19. | Vikat A, Rimpelä M, Salminen JJ, Rimpelä A, Savolainen A, Virtanen SM. Neck or shoulder pain and low back pain in Finnish adolescents. Scand J Public Health 2000;28:164-73. [Google Scholar] |
| 20. | Shan Z, Deng G, Li J, Li Y, Zhang Y, Zhao Q. How schooling and lifestyle factors effect neck and shoulder pain? A cross-sectional survey of adolescents in China. Spine (Phila Pa 1976) 2014;39:E276-83. [Google Scholar] |
| 21. | Silva MR, Badaró AF, Dall'Agnol MM. Low back pain in adolescent and associated factors: A cross sectional study with schoolchildren. Braz J Phys Ther 2014;18:402-9. [Google Scholar] |
| 22. | Harreby M, Nygaard B, Jessen T, Larsen E, Storr-Paulsen A, Lindahl A, et al. Risk factors for low back pain in a cohort of 1389 Danish school children: An epidemiologic study. Eur Spine J 1999;8:444-50. [Google Scholar] |
| 23. | Masiero S, Carraro E, Celia A, Sarto D, Ermani M. Prevalence of nonspecific low back pain in schoolchildren aged between 13 and 15 years. Acta Paediatr 2008;97:212-6. [Google Scholar] |
| 24. | Diepenmaat AC, van der Wal MF, de Vet HC, Hirasing RA. Neck/shoulder, low back, and arm pain in relation to computer use, physical activity, stress, and depression among Dutch adolescents. Pediatrics 2006;117:412-6. [Google Scholar] |
| 25. | Myrtveit SM, Sivertsen B, Skogen JC, Frostholm L, Stormark KM, Hysing M. Adolescent neck and shoulder pain – The association with depression, physical activity, screen-based activities, and use of health care services. J Adolesc Health 2014;55:366-72. [Google Scholar] |
| 26. | Onofrio AC, da Silva MC, Domingues MR, Rombaldi AJ. Acute low back pain in high school adolescents in Southern Brazil: Prevalence and associated factors. Eur Spine J 2012;21:1234-40. [Google Scholar] |
| 27. | Sjolie AN. Persistence and change in nonspecific low back pain among adolescents: A 3-year prospective study. Spine (Phila Pa 1976) 2004;29:2452-7. [Google Scholar] |
| 28. | Auvinen JP, Tammelin TH, Taimela SP, Zitting PJ, Järvelin MR, Taanila AM, et al. Is insufficient quantity and quality of sleep a risk factor for neck, shoulder and low back pain? A longitudinal study among adolescents. Eur Spine J 2010;19:641-9. [Google Scholar] |
| 29. | AlShayhan FA, Saadeddin M. Prevalence of low back pain among health sciences students. Eur J Orthop Surg Traumatol 2018;28:165-70. [Google Scholar] |
| 30. | Torgén M, Swerup C. Individual factors and physical work load in relation to sensory thresholds in a middle-aged general population sample. Eur J Appl Physiol 2002;86:418-27. [Google Scholar] |
| 31. | Wedderkopp N, Andersen LB, Froberg K, Leboeuf-Yde C. Back pain reporting in young girls appears to be puberty-related. BMC Musculoskelet Disord 2005;6:52. [Google Scholar] |
| 32. | O'Sullivan PB, Beales DJ, Smith AJ, Straker LM. Low back pain in 17 year olds has substantial impact and represents an important public health disorder: A cross-sectional study. BMC Public Health 2012;12:100. [Google Scholar] |
| 33. | Balagué F, Skovron ML, Nordin M, Dutoit G, Pol LR, Waldburger M. Low back pain in schoolchildren. A study of familial and psychological factors. Spine (Phila Pa 1976) 1995;20:1265-70. [Google Scholar] |
| 34. | Bener A, Verjee M, Dafeeah EE, Falah O, Al-Juhaishi T, Schlogl J, et al. Psychological factors: Anxiety, depression, and somatization symptoms in low back pain patients. J Pain Res 2013;6:95-101. [Google Scholar] |
| 35. | Bener A, EL-Rufaie OF, Siyam A, Abuzeid MS, Toth F, Lovasz G. Epidemiology of low back pain in the United Arab Emirates. APLAR J Rheumatol 2004;7:189-95. [Google Scholar] |
| 36. | Bener A, EL-Rufaie OF, Kamran S, Georgievski AB, Farooq A, Rysavy M. Disability, depression and somatization in a low back pain population. APLAR J Rheumatol 2006;9:257-63. [Google Scholar] |
| 37. | Niemi SM, Levoska S, Rekola KE, Keinänen-Kiukaanniemi SM. Neck and shoulder symptoms of high school students and associated psychosocial factors. J Adolesc Health 1997;20:238-42. [Google Scholar] |
| 38. | Lusa S, Miranda H, Luukkonen R, Punakallio A. Sleep disturbances predict long-term changes in low back pain among Finnish firefighters: 13-year follow-up study. Int Arch Occup Environ Health 2015;88:369-79. [Google Scholar] |
| 39. | Hakala P, Rimpelä A, Salminen JJ, Virtanen SM, Rimpelä M. Back, neck, and shoulder pain in Finnish adolescents: National cross sectional surveys. BMJ 2002;325:743. [Google Scholar] |
| 40. | Skaggs DL, Early SD, D'Ambra P, Tolo VT, Kay RM. Back pain and backpacks in school children. J Pediatr Orthop 2006;26:358-63. [Google Scholar] |
| 41. | Silva AG, Sa-Couto P, Queirós A, Neto M, Rocha NP. Pain, pain intensity and pain disability in high school students are differently associated with physical activity, screening hours and sleep. BMC Musculoskelet Disord 2017;18:194. [Google Scholar] |
Fulltext Views
3,575
PDF downloads
1,197




