Translate this page into:
Use of dual cup mobility technique with bone grafting for reconstruction of acetabular defect in hip sarcoma without stabilizing plates
2 Reconstructive Orthopedic Department, King Fahad Medical City, Riyadh, Saudi Arabia
Corresponding Author:
Reema M Alhussein
College of Medicine, Dar Al Uloom University, Riyadh
Saudi Arabia
reemaalhusseinn@gmail.com
| How to cite this article: Alhussein RM, Albarrak MM, Alshaya OS. Use of dual cup mobility technique with bone grafting for reconstruction of acetabular defect in hip sarcoma without stabilizing plates. J Musculoskelet Surg Res 2019;3:298-302 |
Abstract
Acetabular reconstruction following malignancy is considered to be a difficult technique regarding the management of severe bone loss. We report a case of pleomorphic undifferentiated sarcoma involving the right femoral head extending to the acetabulum, in a patient presenting with deteriorating right hip pain. We investigated systemically and locally by radiographs, computed tomographic scan, magnetic resonance imaging, and bone scan. We used a modified extra-articular wide surgical resection of the proximal femur and acetabulum instead of classic extra-articular resection followed by reconstructed using cancellous bone chips and dual mobility cup without stabilizing plates. At 6-month follow-up, the allograft had united with the host bone, and radiographs showed satisfactory position and stability of the components. To the best of our knowledge, this scenario has not been reported in other literature. We recommend further studies to be performed in a larger number of patients with longer follow-up to confirm the satisfaction with impaction of bone grafting in a patient with hip sarcoma without stabilizing plates.Introduction
Acetabular reconstruction following malignancy is considered to be a difficult technique.[1] Obtaining stability and long-standing fixation are the main purpose of this procedure. However, one of the major challenges in such cases is dealing with severe acetabular deficiency.[2] Various approaches have been adopted to maintain the stability and to manage the deficiencies. One of the approaches is using impaction bone grafting (IBG) in combination with cemented socket without using reamer in reverse to impact the grafts.[3] A study was done in Freeman Hospital involved 24 patients who underwent complex reconstruction of the acetabulum with the use of trabecular metal augments in filling the bone defect and provided a stable foundation for IBG. It showed to be an effective method in addition to providing a stable foundation for IBG with favorable outcome and low failure rate with follow-up for a median of 5 years.[4]
To the best of the authors' knowledge, no reports so far have been found of using bone grafting in addition to dual mobility cup (DMC), without using stabilizing plates in a patient with hip sarcoma.
Case Report
A 31-year-old female patient presented to the orthopedic screening clinic on a wheelchair with a 4-month history of deteriorating right hip pain. It was gradual in onset, started as mild pain, then progressed, and radiated to the right knee. The patient could not walk freely and perform daily living activities with no pain. In the last 2–3 months, she was unable to bear weight. The patient's medical history was uneventful. She denied a history of trauma, previous fracture, or constitutional symptoms.
Physical examination revealed mildly swilling over the right hip associated with tenderness and redness. There was limitation of the range of motion in the hip due to pain. She had a 2-cm shortening over the affected side. Her ability to bear weight was impeded by hip pain. Distal neurovascular examination was normal.
Radiographs of the pelvis revealed the presence of a pathological fracture in the right femoral neck [Figure - 1]. Local and systemic evaluation did not show any pathology or distant metastasis. Magnetic resonance imaging (MRI) demonstrated an intertrochanteric fracture of the right femoral neck associated with large enhancing soft tissue mass infiltrating the bone marrow [Figure - 2].
![[Figure - 1]](#fig_SaudiOrthopJ_2019_3_3_298_253803_f1.jpg){kind=link}
![[Figure - 2]](#fig_SaudiOrthopJ_2019_3_3_298_253803_f2.jpg){kind=link}
 |
| Figure 1: Anteroposterior (AP) pelvis radiograph demonstrating pathological fracture in the right femoral neck |
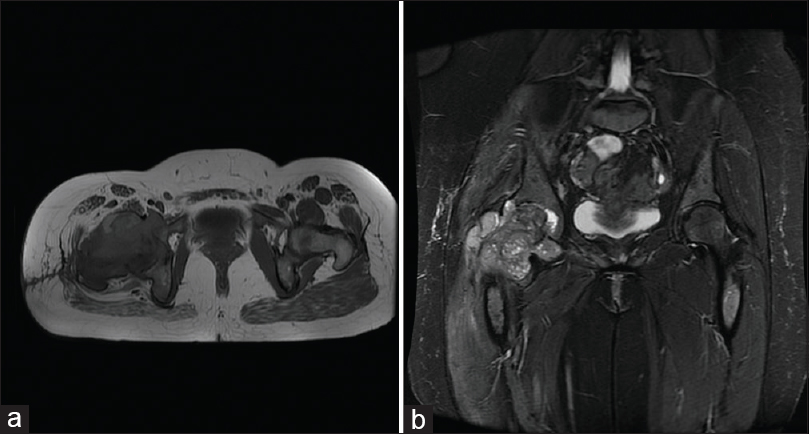 |
| Figure 2: (a) Axial and (b) coronal T2-weighted magnetic resonance imaging without contrast revealed a large aggressive soft tissue lesion at proximal femur involving femur neck measured 9.4 cm × 7.7 cm × 8 cm. A 1 cm of prominent lymph node was noted in the right iliac |
On additional evaluation, she underwent whole-body scintigraphic bone scanning, which showed increased focal uptake over the fracture [Figure - 3]. CT-guided biopsy of the mass was done and repeated after 6 weeks, they both were reviewed by several pathologists in Riyadh, and they all agreed that they were inconclusive. Another open biopsy was taken. The initial histopathological examination of the surgical specimen suggested the presence of high-grade undifferentiated pleomorphic sarcoma with spindle cells. The tumor was grade 2B second stage. We started her on neoadjuvant chemotherapy of ifosfamide and doxorubicin. The patient did not undergo radiation. After six cycles, the MRI showed a decrease in tumor size [Figure - 4]. A decision was made for surgical resection.
![[Figure - 3]](#fig_SaudiOrthopJ_2019_3_3_298_253803_f3.jpg){kind=link}
![[Figure - 4]](#fig_SaudiOrthopJ_2019_3_3_298_253803_f4.jpg){kind=link}
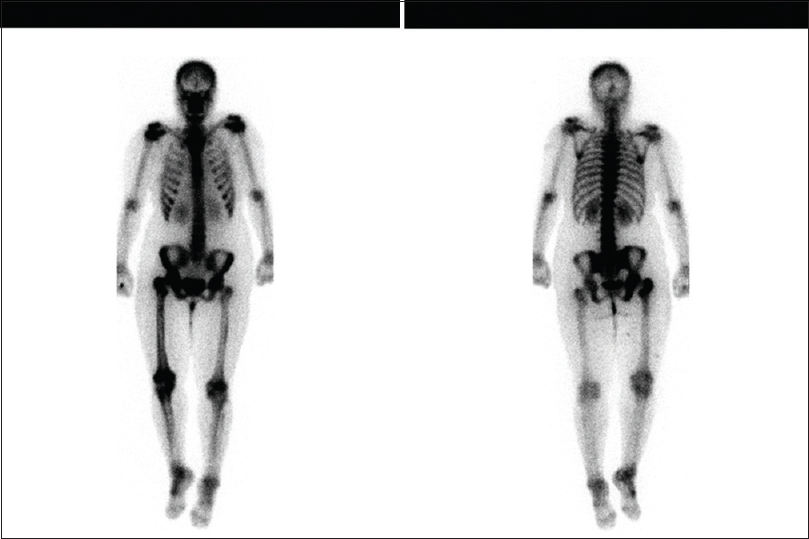 |
| Figure 3: Bone scan done using Tc.99M showing increase focal uptake over the fracture in the intertrochanteric region of the right femur, but it was negative for multifocal metastatic disease |
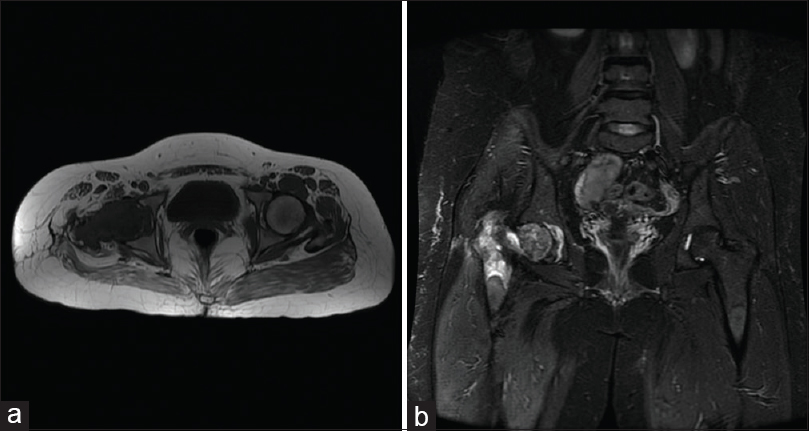 |
| Figure 4: Axial (a) and coronal (b) T2 magnetic resonance images reveal a decrease in tumor size to 3.6 cm × 7.3 × 6 cm |
Surgical procedure
Global modular replacement system ® system by STRYKER ® was used during the procedure. The patient was placed on lateral position. The hip joint was exposed using the posterolateral approach. First, an incision was made around the old biopsy to resect the tumor as a modified extra-articular En Bloc resection instead of a classic extra-articular resection by cutting about 12 cm at the proximal femur and a 2 cm margin around the acetabular side, where zone 2 was resected carefully. The resected soft tissue and bony mass were sent to the laboratory for margin examination and came back to be negative [Figure - 5].
![[Figure - 5]](#fig_SaudiOrthopJ_2019_3_3_298_253803_f5.jpg){kind=link}
 |
| Figure 5: Resected of soft tissue and bony mass were sent to the laboratory for margin examination |
The periacetabular resection was done using fluoroscope and multiple K-wire around the acetabulum. Then, the graft was placed based on the shape of anterior and posterior columns where the resection happened in cone shape. It was made by removing the medial wall while maintaining the anterior and posterior columns and remnant of medial cortex of medial wall, to give the containment, where the allogeneic cadaveric cancellous bone graft 45 CCs was placed. Afterward, the graft was washed with water and 2 g of cefazolin and we used a reverse reamer to give the containment the shape needed. A thorough wash was done with sterile water, hydrogen peroxide, and betadine. Megacup size 64 mm was placed. It was fixed with three screws measured 6.5 mm to the inferior ilium, which gave the press-fit shape where we were able to put the constrained cup on it, size 28 mm. The reconstruction of the proximal femur was started; cemented stem was used size 11 mm × length of 127 mm with an extension piece length of 40 mm. A proximal femoral component measuring 28 mm was implanted. Repeated thorough irrigation and debridement with sterile water, hydrogen peroxide, and betadine was done [Figure - 6].
![[Figure - 6]](#fig_SaudiOrthopJ_2019_3_3_298_253803_f6.jpg){kind=link}
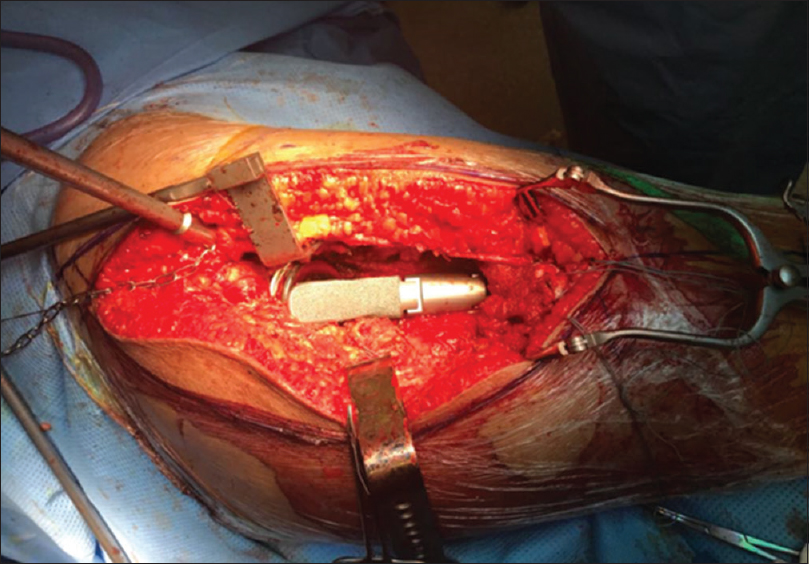 |
| Figure 6: Intraoperative photograph after replacing the proximal femur and acetabulum |
The operation was finished using the short rotators of the proximal hip, heavy sutures mersilene tape, number 2 fiber wire, and the premade holes within the proximal femur prosthesis to close it. Then, a tube was used within the proximal femur to close the proximal femur short rotators cuffs and abductor muscles within the proximal prime hole of proximal prosthesis. Using sheath and synthetic tube, the abductor muscle was held to the remnant of rectus femurs anterior, and the short rotators to abductor muscle to the proximal part of prosthesis to suture the remaining of the tissue. Skin layers were closed with staples.
Total operating time was 5 h, blood loss was around 1000 ml, and the patient received 600 ml packed red blood cell intraoperative.
Outcome and follow-up
During her 2-day hospitalization, there was no recorded postoperative complication. Right-sided nonweight-bearing protocol was initiated for 6 weeks after she was seen and assessed by the physiotherapy team. Two weeks later at her follow-up, the wound was healed with no complications. One month following her surgery, she went back to adjuvant chemotherapy. Six weeks after the operation, we started her with partial weight bearing for 4 more weeks. She was finally advanced to full weight bearing 10 weeks postoperation, with better balance and increased range of movement. At 7-month follow-up, pelvic radiographs and CT scan were done [Figure - 7] and [Figure - 8].
![[Figure - 7]](#fig_SaudiOrthopJ_2019_3_3_298_253803_f7.jpg){kind=link}
![[Figure - 8]](#fig_SaudiOrthopJ_2019_3_3_298_253803_f8.jpg){kind=link}
 |
| Figure 7: Anteroposterior (AP) pelvis radiograph revealed status post total right hip replacement showing the acetabular prosthesis is place fixed by screws and added cement material |
 |
| Figure 8: Axial contrast-enhanced computed tomography image revealed satisfactory position of the components |
Discussion
Different reconstruction techniques have been obtained for periacetabular tumor lesions that may exist in different areas of the acetabulum with a variation in size.[1],[2] Since these lesions present with extensive loss of bony support, it poses a challenge among orthopedic surgeons.[5] van Haaren et al. linked the higher failure rate with insufficient experience of surgeons.[6] Other studies considered the size of bone loss as a major predictor for operation failure.[7],[8] A case–control study found an increase hip dislocation rate was associated with tumor resection due to different factors as bone loss and tissue compromise.[9]
Various techniques have been in use, to enhance bone stability. These techniques include introducing larger bone graft size and prior washing of the graft. It has shown that washing before impaction can increase the shear strength of the graft and therefore improve the mechanical stability of the acetabular component.[10],[11] Implanting buttress plate is another technique that has been shown to add structural support and further stability to the graft.[12],[13]
A study done by Comba et al. reported that patients who have done IBG with cemented components had a 95.8% survival rate after 51.7 months.[14] In addition, IBG using both cemented and cementless techniques was a successful technique in achieving acetabular reconstruction and provided stability to the acetabulum component.[15]
A study by van Haaren et al. reported high rates of failure in IBG. The study reviewed 71 cases of revision THA, 20 patients from the 71 cases needed a re-revision resulting in a 72% survival rate. The authors considered that the high rate of failure was related to the insufficient experience and a high prevalence of segmental acetabular defects.[6]
In our case, the patient was followed up for a short-term for 7 months. She showed well integration of bone graft within the cup. She was able to walk without assistant, pain, or limited range of motion. The patient is scheduled to have 6 months follow-up.
We did not use three-dimensional navigation as it is not available in our institution, but these kinds of procedures are better to be done under navigation. In addition, we concur that this case report will serve as an interim report, as we aim to follow-up the patient for long term results.
Conclusion
Using the bone graft followed by reconstruction with DMC without stabilizing plates considered a successful procedure in our oncology case. It had shown favorable outcomes for 7 months follow-up and allowed the patient to return to normal weight bearing at about 3 months postoperation without complications. Further studies are suggested, to evaluate long-term outcome of this technique.
Ethical approval
This study has been approved from our institution's IRB committee and written informed consent was received from the patient for publication of this case report and accompanying images.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
Authors' contribution
OSS designed the study, provided research materials and provided logistic support. RMH and MMB gathered the information and wrote the initial and final draft of the article. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index.
| 1. | Brown TS, Salib CG, Rose PS, Sim FH, Lewallen DG, Abdel MP, et al. Reconstruction of the hip after resection of periacetabular oncological lesions: A systematic review. Bone Joint J 2018;100-B:22-30. [Google Scholar] |
| 2. | Shon WY, Santhanam SS, Choi JW. Acetabular reconstruction in total hip arthroplasty. Hip Pelvis 2016;28:1-4. [Google Scholar] |
| 3. | Welten ML, Schreurs BW, Buma P, Verdonschot N, Slooff TJ. Acetabular reconstruction with impacted morcellized cancellous bone autograft and cemented primary total hip arthroplasty: A 10-to 17-year follow-up study. J Arthroplasty 2000;15:819-24. [Google Scholar] |
| 4. | Borland WS, Bhattacharya R, Holland JP, Brewster NT. Use of porous trabecular metal augments with impaction bone grafting in management of acetabular bone loss. Acta Orthop 2012;83:347-52. [Google Scholar] |
| 5. | van Egmond N, De Kam DC, Gardeniers JW, Schreurs BW. Revisions of extensive acetabular defects with impaction grafting and a cement cup. Clin Orthop Relat Res 2011;469:562-73. [Google Scholar] |
| 6. | van Haaren EH, Heyligers IC, Alexander FG, Wuisman PI. High rate of failure of impaction grafting in large acetabular defects. J Bone Joint Surg Br 2007;89:296-300. [Google Scholar] |
| 7. | Wegrzyn J, Pibarot V, Jacquel A, Carret JP, Béjui-Hugues J, Guyen O, et al. Acetabular reconstruction using a Kerboull cross-plate, structural allograft and cemented dual-mobility cup in revision THA at a minimum 5-year follow-up. J Arthroplasty 2014;29:432-7. [Google Scholar] |
| 8. | Jaiswal PK, Aston WJ, Grimer RJ, Abudu A, Carter S, Blunn G, et al. Peri-acetabular resection and endoprosthetic reconstruction for tumours of the acetabulum. J Bone Joint Surg Br 2008;90:1222-7. [Google Scholar] |
| 9. | De Martino I, Triantafyllopoulos GK, Sculco PK, Sculco TP. Dual mobility cups in total hip arthroplasty. World J Orthop 2014;5:180-7. [Google Scholar] |
| 10. | Bolder SB, Schreurs BW, Verdonschot N, van Unen JM, Gardeniers JW, Slooff TJ, et al. Particle size of bone graft and method of impaction affect initial stability of cemented cups: Human cadaveric and synthetic pelvic specimen studies. Acta Orthop Scand 2003;74:652-7. [Google Scholar] |
| 11. | Arts JJ, Verdonschot N, Buma P, Schreurs BW. Larger bone graft size and washing of bone grafts prior to impaction enhances the initial stability of cemented cups: Experiments using a synthetic acetabular model. Acta Orthop 2006;77:227-33. [Google Scholar] |
| 12. | Sierra RJ, Mabry TM, Sems SA, Berry DJ. Acetabular fractures: The role of total hip replacement. Bone Joint J 2013;95-B:11-6. [Google Scholar] |
| 13. | Okano K, Miyata N, Enomoto H, Osaki M, Shindo H. Revision with impacted bone allografts and the Kerboull cross plate for massive bone defect of the acetabulum. J Arthroplasty 2010;25:594-9. [Google Scholar] |
| 14. | Comba F, Buttaro M, Pusso R, Piccaluga F. Acetabular reconstruction with impacted bone allografts and cemented acetabular components. J Bone Joint Surg Br. 2006;88-B(7):865-9. doi:10.1302/0301-620x.88b7.17227. [Google Scholar] |
| 15. | Ibrahim MS, Raja S, Haddad FS. Acetabular impaction bone grafting in total hip replacement. Bone Joint J 2013;95-B:98-102. [Google Scholar] |
Fulltext Views
2,648
PDF downloads
1,650




