Translate this page into:
Usefulness of immersive virtual reality simulation during femoral nail application in an orthopedic fracture skills course
2 Department Head of Pediatric Orthopaedics, Legaria Children's Hospital, AO Trauma Mexico Committee Chairperson, Mexico City, Mexico
3 Polytrauma, Pelvis and Acetabulum Service Specialty at Occident National Medical Center, IMSS, Education Board Member for AO Trauma Mexico, Guadalajara, Jalisco, Mexico
4 Department Head of Neurological Rehabilitation, National Rehabilitation Institute, Luis Guillermo Ibarra Ibarra, Mexico
Corresponding Author:
Claudia Arroyo-Berezowsky
Av. Vasco De Quiroga #4299, Consultorio 1003, Lomas De Santa Fe, 05348 Cuajimalpa de Morelos, Cd Mx
Mexico
dra.carroyob@gmail.com
| How to cite this article: Arroyo-Berezowsky C, Jorba-Elguero P, Altamirano-Cruz MA, Quinzaños-Fresnedo J. Usefulness of immersive virtual reality simulation during femoral nail application in an orthopedic fracture skills course. J Musculoskelet Surg Res 2019;3:326-333 |
Abstract
Objectives: There is an increasing number of complex and varied surgical techniques and implants in orthopedic trauma. As the paradigm shift in orthopedic surgical education is turning to competency-based curricula and technology is becoming more affordable, new immersive virtual reality (IVR) simulation systems are emerging. The main objective of this study was to evaluate the utility of IVR simulation for learning a complex surgical technique; the application of a Trochanteric Femoral Nail Advanced (TFNA™). Methods: Ten residents participated in the evaluation of the application of TFNA™ in a Synbone® model during an advanced fractures treatment course. Five of them had a previous practice session using a VR simulator to learn the technique. All of them applied a TFNA™ during the course and were then asked to repeat it. Time to completion and the number of steps completed by each group were compared between both groups. Results: The VR group took 25.84 min to complete (standard deviation [SD] 6.14) and the control group 31.6 min to complete (SD 19.3). There was no statistically significant difference between both groups, but there was a tendency for the VR group to complete more steps and finish earlier than the control group (P = 0.554). Conclusion: IVR simulation could be a more accessible way to provide a safe environment where participants can learn a new surgical technique. It is important to develop proficiency-based progressive training programs with specific educational goals that incorporate simulation and emerging technology as a tool. Larger, randomized, internal and external validation studies are needed.Introduction
In the last few years, there has been an increase in simulation research in orthopedics, especially for the development of motor skills. This started due to several limitations in residency programs worldwide, such as restrictions in working hours, higher operating room costs, and more complex procedures.[1] Some of the available kinds of simulators in orthopedics include cadaveric simulation, the use of bench models, and virtual reality (VR) simulation. Camp et al. demonstrated that an arthroscopic VR simulator was more cost-effective than a cadaveric lab for the development of basic arthroscopic skills.[2] Most research and technology development done in simulation in orthopedics has focused on motor skill improvement in arthroscopy, since arthroscopy is a surgical technique amenable to simulation.[1],[3]
The current consensus in orthopedics and other surgical subspecialties is that there needs to be a paradigm shift in surgical education, where simulation-based training is incorporated into the curricula.[4] The downside to this is that curricula and program development have fallen behind and measurement techniques that ensure a certain level of proficiency are not well defined.[5]
Almost all VR arthroscopic simulators are built as a unit that includes a screen, two robotic arms where instruments can be added that resemble real-life instruments, and a knee, shoulder, or even a hip model that can be switched out. Technology has been developed around haptic feedback from the robotic arms to simulate the sensations during a real arthroscopic surgery. Software is used to recreate the inside of a joint, and it allows for the user to perform a specific surgery. Most of these simulators measure certain metrics such as distance traveled, time to complete tasks, and roughness. These metrics have been found to discriminate between novice and expert users, but there is difficulty discriminating between intermediate trainees.[6],[7]
As mentioned before, most of the interest in simulation in orthopedics has focused on arthroscopic simulators. There are only few simulators available for orthopedic trauma procedures.
Some of the first simulation activities for orthopedic trauma were fracture treatment skills courses such as those pioneered by the AO Foundation (Trauma division) where participants practice certain surgical skills such as drilling and fracture fixation under the supervision of experienced faculty.[1],[8] Egol et al. demonstrated in 2015 that participation in such formal surgical skills courses significantly improved practical operative skills as assessed by simulation in synthetic bone models. The benefits of the course were maintained for 6 months 6 months in synthetic bone models. No external validation was assessed for transferability to the operating room.[8] One of the most recent simulators for orthopedic trauma procedures is a mobile device application (app) called Touch Surgery. With this application, the user focuses on learning the steps to perform a specific surgical technique, developing cognitive skills instead of the motor skills needed.[9]
The available VR simulators for orthopedic trauma resembled the arthroscopic VR simulators; they consisted of a monitor and robotic arms with or without an anatomical model and software to recreate the surgery. Some even focused on haptic feedback like arthroscopic simulators.[10],[11]
As technology is becoming more advanced, more affordable, and more user- and developer-friendly, simulation in orthopedics is taking a new direction. The most recent technological advance for orthopedic trauma VR simulation is the development of immersive VR simulators (IVRs) that take advantage of existing commercial technology available for personal use. Wearing a headset, the user becomes engaged in an environment that resembles an operating room. With the use of commercial handles, the user can manipulate instruments in the virtual operating room in order to learn and complete a surgical technique. Another difference with previous VR simulation is the development of implant- and procedure-specific software. Such an IVR simulator became available in Mexico this year. The available software includes three procedures. One of these modules involves the application of a trochanteric femoral nail. We used this simulator for a pilot study during advanced principles of fracture treatment course in Mexico City, where the application of the same trochanteric femoral nail would be part of the practical exercises.
The main objective of this study was to evaluate the utility of VR simulation for learning the steps for a complex surgical technique involving the application of a trochanteric femoral nail.
Materials and Methods
For this study, we used the IVR simulator for Trochanteric Femoral Nail Advanced (TFNA™) ©DePuy Synthes (Johnson and Johnson) application developed by Pixelmolkerei (Pixel Dairy Productions Inc., -Switzerland) for the Johnson and Johnson Institute for use with the Samsung Odyssey hardware (Samsung-Korea) [Figure - 1].
![[Figure - 1]](#fig_SaudiOrthopJ_2019_3_4_326_270871_f1.jpg){kind=link}
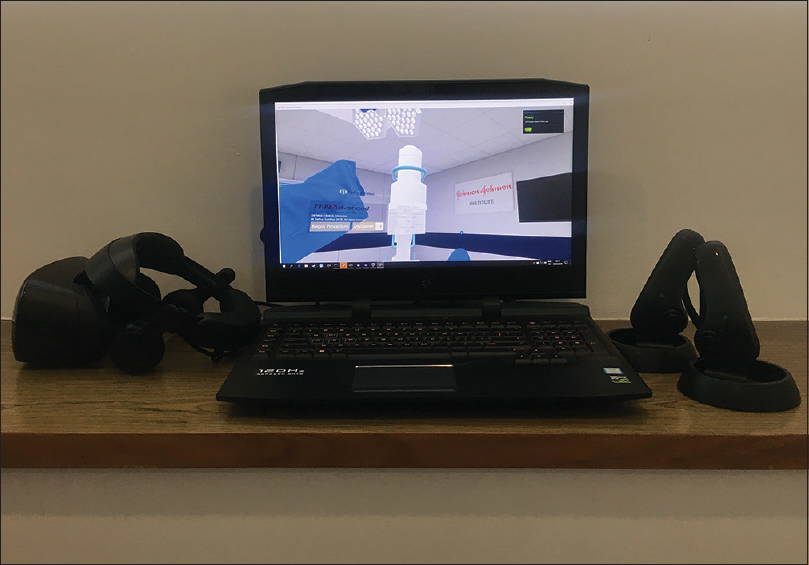 |
| Figure 1: Immersive virtual reality simulator with gaming laptop and Samsung Oddyssey lens and controllers |
The simulator software includes a module for primary total knee arthroplasty, a module for the application of the TFNA™ (with the possibility of using a blade, a screw or augmentation) and a module for anterior hip approach. The user wears the headset to visualize the simulated environment. This is an operating room where the user is positioned as the surgeon and has an instrument table available. When the TFNA™ module is launched, the patient appears positioned on the fracture table, already draped, and prepped for the operation of a right trochanteric fracture. There is an image intensifier in the operating room and some steps require visualization of predefined X-ray imaging. The surgeon must complete every step (there are no assistants, operating room technicians, or scrub nurses), including the assembly of the instruments required to position the TFNA™. The module runs from the incision for the surgical approach through the placement of the TFNA™, and it ends when the nail is correctly placed and the handle is disassembled. There is no simulation for fracture reduction.
All the necessary instruments to complete the surgery are placed on two tables located to the right and back of the surgeon. If the user is doing the exercise with help, the instruments needed for each surgical step are highlighted in white, and some specific instructions appear on the screen (how to turn a knob or how to assemble the handle). The Samsung Odyssey controllers are used to manipulate instruments and vibrate when the right step is completed, or the right instrument is grabbed. You can visualize the ghost controllers inside the simulation instead of the surgeon's hands. Time to completion is measured for the total surgery and for different action blocks within the procedure. The user can complete the module with or without help. If the no help mode is selected, instruments are not highlighted nor any instructions given. The participant has to complete every step with the right sequence and hand position to move forward. There are no metric measurements other than the time to complete the exercise, and no summary is offered at the end of the simulation.
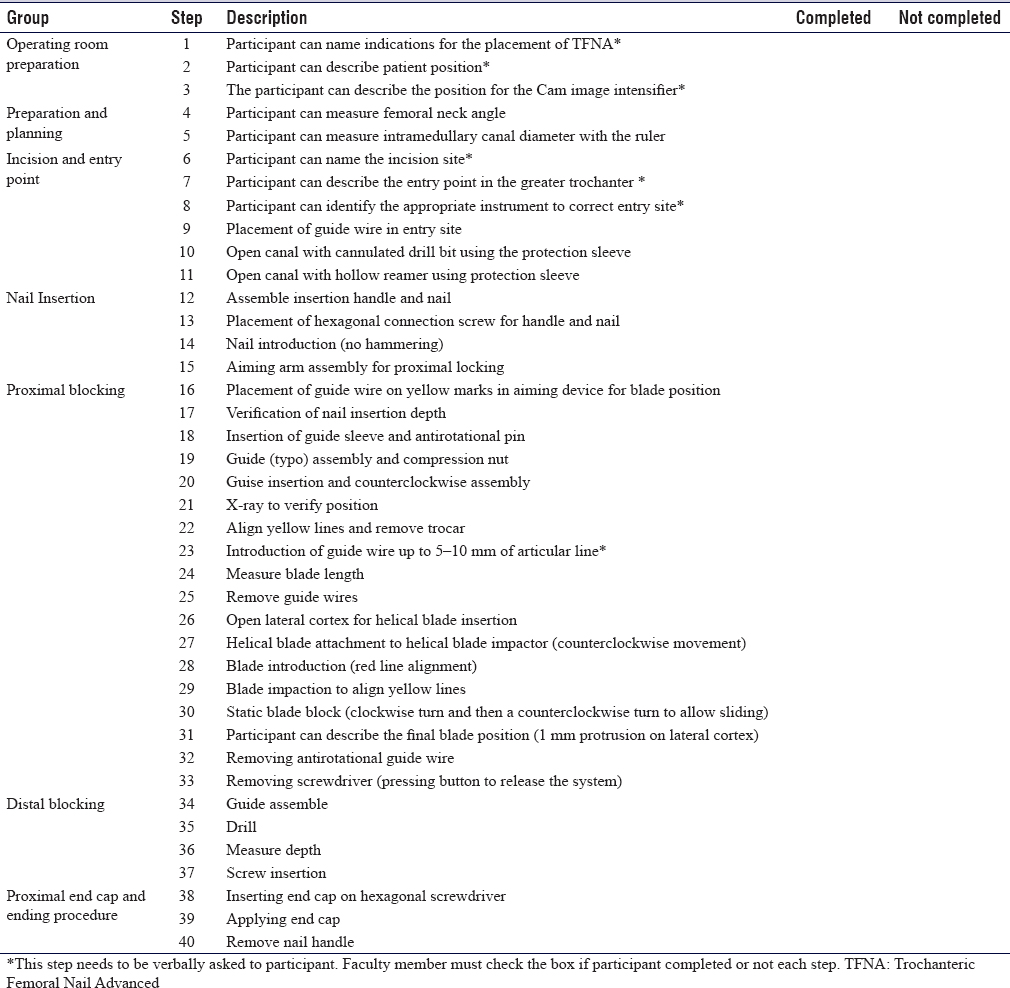
Since there are no metrics and a measure of the participant's performance was needed, a checklist designed where the steps for application of the implant were specified was designed. For this, we reviewed the implant's brochure with the surgical technique, the whole simulation sequence, and the video used during the AO trauma advanced principles fracture course. The checklist includes two important parts: Operating room preparation and nail insertion. We divided the whole sequence into nine main stages: indications for TFNA™, patient positioning, preparation and planning, incision and entry site preparation, nail insertion, proximal blocking, distal blocking, end cap insertion, and handle removal. There were a total of 40 individual steps. Eight of these steps need to be asked to the participant to assess the dominion. The checklist is structured as a yes/no questionnaire. The checklist can be seen in [Table - 1].
![[Table - 1]](#tbl_SaudiOrthopJ_2019_3_4_326_270871_t2.jpg){kind=link}
Proximal femur Synbone® model LD2220 was used for the application of the TFNA™ during the course and in the final evaluation.
During the advanced principles of fracture treatment course that took place in Mexico City, we invited ten residents who were enrolled in the course to participate in our study. All residents participated voluntarily. They all signed a consent form and filled a questionnaire with demographic information. Participants were divided into two groups, but they were not randomized. The five participants who were able to attend to the VR session before the course started were allocated to the VR group. The other five residents were allocated to the control group.
The VR group had 1 h to freely work with the simulation program for the TFNA™ with a static blade (exercise 1 of the TFNA™ module). During the simulation, the user completed the whole sequence for the application of the TFNA™, including the assembly before insertion in the femoral canal. This simulation could either be done with visual aids to identify the material needed in each step and the position of the instruments or without aids. When no aids were used, if the user did not do the adequate sequence and place the instrument in the correct position, he or she could not advance to the next step of the surgery. Participants received a small briefing on how to use the VR simulator from the main author. Then, they were free to do the simulation with or without help. Most of them started with help and progressed until they could do it without help.
On that same day, during the advanced principles of fracture treatment course, all ten participants were involved in skills exercise, during which, they watched a video with instructions on how to place the TFNA™, after which they placed it on a Synbone® model.
The next day, all participants had an hour to place the TFNA™ without assistance. Faculty members used the checklist to assess the completion of the exercise. Some of the steps needed to be asked to the participants in order to assess them. No help was given to complete the procedure. The faculty members also recorded the time for completion of the exercise.
Time to completion of implant application was compared between groups. The number of steps completed by all participants was also compared between both groups.
Statistics
Statistical analysis consisted of normality tests for continuous variables (Kolmogorov–Smirnov and Shapiro–Wilk test). Quantitative parametric variables were described as medians (standard deviation [SD]) and nonparametric variables as means (interquartile range, minimum-maximum). Qualitative variables were described as frequencies.
Comparisons between parametric numeric variables were made with Student's t-test for the parametric and of Mann–Whitney U-test for the nonparametric variables. Medians are reported with a 95% confidence interval. A two-tailed P < 0.05 value was considered statistically significant.
Results
There were ten participants. Four of them were female and six male. There were seven postgraduate year-4 (PGY4) residents and three PGY3. Four of them were from the same institution, three more were from another hospital and the rest were from a different hospital each. The median age of the participants was 28.6 years [Table - 2].
![[Table - 2]](#tbl_SaudiOrthopJ_2019_3_4_326_270871_t3.jpg){kind=link}
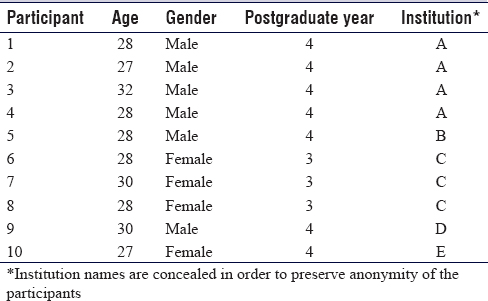
All of them were familiar with the TFNA™ before the fractures course. Seven of them had read the application technique for the TFNA™ before, six had watched a video about the surgical technique, and five had assisted in a surgery where the TFNA™ was applied. Three of them had applied a TFNA™ with assistance and none had applied it as a lead independent surgeon. Six participants mentioned there had been a technician in the operating room when they had applied the TFNA™. Regarding preoperative planning, eight of the residents said that they did a preoperative plan before choosing an implant; eight of them also did preoperative planning before going into surgery. All of them thought simulation could help learn and improve a surgical technique, and all of them said that they would use the simulator if they had access to it.
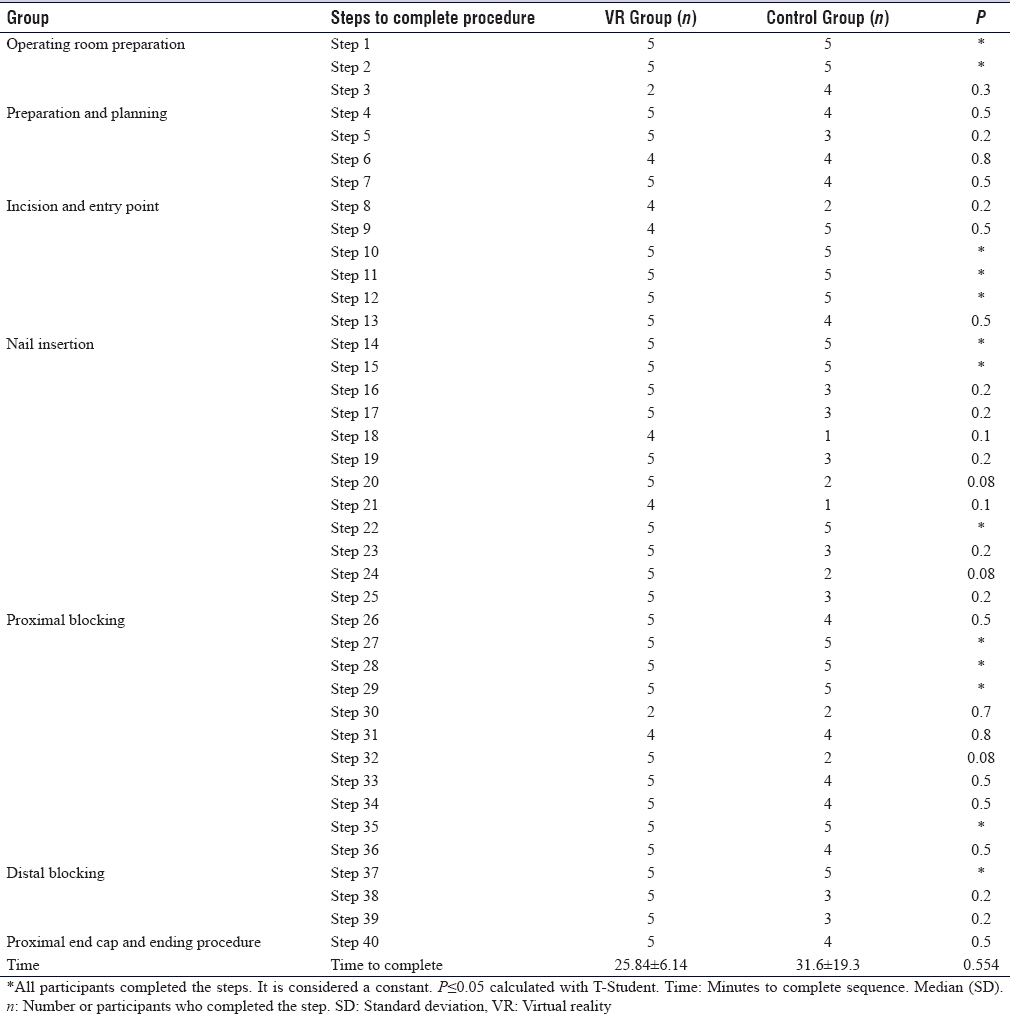
There was one faculty member who did not record time to completion, so the registry for one of the control group participants was missing. The VR group had a median of 25.84 min to completion (SD 6.14 min) and the control group 31.6 min (SD 19.3 min). There was no statistically significant difference between both groups (P = 0.554), although there was a tendency for the VR group to perform faster.
The checklist was divided into seven sections: Operating room preparation, preoperative planning, incision and entry site identification, TFNA™ introduction, proximal locking with a spiral blade, distal locking, and end cap insertion [Table - 1]. There were a total of 40 different steps for applying TFNA™. Thirteen of these steps were completed by all participants and were hence considered as a constant step. There were no statistically significant differences between both groups. However, there was a tendency for patients in the VR group to have a better outcome, especially during steps 8, 16–21, 23–25, 32, 38, and 39. More participants in the control group than in the VR group completed step 3 (this step is not included in the VR simulation and was only mentioned in the video) [Table - 3].
![[Table - 3]](#tbl_SaudiOrthopJ_2019_3_4_326_270871_t4.jpg){kind=link}
Male residents tended to complete the sequence in less time than female residents (28.8 min ± 9.2 min vs. 20.25 min ± 24.63 min), although this difference was not statistically significant. However, all female residents belonged to the control group, so we do not believe gender had any influence in performance.
A subanalysis was also made regarding the level of training. PGY4 residents took less time than PGY3 residents to complete the sequence R3 (24.7 ± 13.8 vs. 27 ± 25.2 min). Again, this was not statistically significant (P = 0.85). And, again, all PGY3 residents belonged to the control group. All PGY4 residents managed to complete step five and only one PGY-3 resident completed it (P = 0.01). There was a tendency for PGY4 residents to have a better performance than PGY3 residents, although this was not statistically significant.
Discussion
Surgical fracture skills courses are the ultimate simulation experience. In 1990, Aderson defined that psychomotor learning cannot be isolated from the cognitive dominion. The individual attempting to develop a specific motor skill must have theoretical information about the ability he or she is to develop.[12] During AO trauma courses, there are specific moments to develop motor skills such as fracture reduction, drilling, and implant application, and other moments where cognitive training with clinical case analysis and decision making are encouraged, while feedback from faculties is obtained. The whole course is structured to balance both motor and cognitive skill acquisition. The educational value of these courses has been demonstrated by Egol et al. in 2015[8] and is recognized in such way, that attendance to these kinds of courses has become a mandatory part of training during trauma and orthopedic residencies in certain countries.[13]
There are no studies that demonstrate that a single participation during a trauma course can help the participant learn a complex surgical technique. Various studies have looked into the time it takes to achieve competency in orthopedic procedures.[14],[15] Bjorgul et al. found that residents needed 20 unlocked and 30 locked femoral nailing procedures to perform faster than their first five procedures.[15] Gustafsson et al. propose that time needed to train to reach a plateau in a learning curve varies from person to person. They established a pass/fail system based on learning curves graded by a score determined by metrics measured by the VR simulator they used, comparing expert surgeons and novice residents. They recommend that trainees should be expected to train to achieve expert proficiency level and that lower standards should not be encouraged.[16] It has also been demonstrated that an inexperienced surgeon has significantly worst outcomes than an experienced one.[15],[16]
In this pilot study, we studied ten residents who attended an AO Trauma advanced principles of fractures course in Mexico City. All of them had participated in surgeries involving the application of TFNA™ but had never done it as independent surgeons. The group who had access to the IVR simulation and had free time to analyze and complete the exercise on their own performed faster and completed more steps. These steps include very specific gross motor knowledge on the application technique for this particular nail, such as which way to turn the knobs on the handles and how to assemble the nail for its introduction and blocking. This could further support what has been consistently proposed about the advantages of VR simulation as an effective way to establish the initial part of a training curve for an inexperienced surgeon or trainee in a safe environment outside the operating room.[16] It has been demonstrated that residents trained with VR tend to perform surgery faster than those with only conventional training.[10] Bjorgul et al. observed in a clinical study that there was a significant correlation between the number of cases completed by a resident and the decrease in operating time.[15] They are also less likely to damage tissues, cause injury, or fail to progress during a specific surgery when trained with VR as demonstrated in laparoscopic surgery.[17]
While our sample was small, and there were no statistically significant differences between both groups in time to complete the exercise and number of steps completed, we did observe a trend toward the IVR group to perform faster and complete more steps. The only step that the control group completed more times was the position of the C-arm. It is interesting because this step was only mentioned during the video at the practical exercise. We believe that residents in the IVR group felt confident enough that they knew the surgical technique and did not pay enough attention to instructions given in the video. This shows that it is as important to know the theoretical aspects as well as how to perform the task. Using the simulator is not a substitute for studying the surgical technique, and only paying attention to an explanation on the surgical technique is not enough to learn it.
With the upsurge of VR and other forms of simulation, as well as proficiency-based programs, it has become clear that an effort needs to be made to develop specific plans that include progressive training. Only using simulators will not predict skill acquisition.[18] Simulators have been used both as training and as assessment tools.[19] While competency based-curricula are gaining momentum and interest around the world, and some countries such as Canada, the United States, and the United Kingdom have adopted simulation as a form of competency training, two main problems remain. Access to simulation labs and simulators is restricted because of the expense and training programs do not have adequate assessment practices. Most feedback for trainees is usually restricted to verbal, informal feedback.[13] It is also our responsibility as physicians to help develop these progressive programs together with the right assessment and feedback tools, since technological development of simulators, and specifically, VR simulators has focused more on resembling a procedure than establishing specific learning goals.[13],[18]
Experience in orthopedic trauma simulation is very limited regarding VR simulators. Traditionally, bench models and synthetic bones have been used to practice and learn osteosynthesis principles as part of the fractures courses. These have the advantage of actually being able to see what happens when you drill and place a screw.[8] However, reusable implants for practicing and the equipment needed to place them are not usually available for routine use. Not even in hospitals with access to skills labs. In a review by Vaughan et al. of VR-based training simulators for orthopedic surgery, they found 11 hip replacement preoperative planning tools, 9 hip trauma fracture simulators, 9 knee arthroscopy simulators, and 8 varied orthopedic simulators available to 2016.[10] Of these nine hip trauma simulators, four were for placing a dynamic hip screw and the rest for drilling and guide placement. None of these include a complete surgical procedure and not a single VR simulator for the placement of a femoral nail has been studied.[10] The IVR simulator we used focuses more on the development of cognitive skills and general knowledge of the implant application technique. While there is a motor component because the simulation is completely immersive and the user needs to handle instruments, the objective is that the user becomes familiar with the instrumentation process.
The only validated cognitive task simulation we found for the application of a femoral nail was Touch surgery™ application (app). This app demonstrated construct, face, and content validity. This way, the users can demonstrate cognitive competencies before performing an actual procedure in the operating room. The authors suggested that it has the potential for curricular implementation.[9] The IVR simulator used in this study is designed more like a cognitive simulator with a gross motor component, than a purely motor simulator. It is similar in some ways to the Touch Surgery™ app. However, this VR simulator is immersive and brings the user into the actual operating room with a real patient setup. While the user can manipulate the instruments through the Samsung Odyssey controllers and they vibrate, they do not offer haptic feedback or anything resembling real sensitivity during the procedure. The main objective is that the user learns the steps of the application technique with very specific motor components, such as the direction the screws or handles need to be turned to. The greatest downside is that it does not measure any metrics, unlike most arthroscopic VR simulators. This makes it difficult to assess performance and improvement. That is why we designed the questionnaire and measured completion time. This questionnaire needs to be internally validated both with intra- and interobserver studies. This will be one of the next steps toward designing a proficiency-based simulation plan for the treatment of trochanteric fractures with intramedullary nailing.
To our knowledge, this is the first study published with this kind of IVR simulator, although it is not the only one available. Another company working on VR simulation for orthopedics and trauma (OSSO VR, Palo Alto, California) has published on its website that a pilot study showed that trainees who trained with IVR performed an anterior hip approach in surgery twice as well as those who were not. However, we were not able to find this study published anywhere.[20] Upon further investigation, the company's CEO mentioned the study is currently under peer review.[21]
This was a pilot study during an advanced principle of fracture treatment course. We observed a tendency toward a better performance and understanding of the surgical technique in participants who were able to practice using the IVR even when the other group also had the opportunity to learn the surgical technique and place the TFNA™ during the fractures course. There were some logistic difficulties we had to overcome, and therefore, could not have a larger sample or a randomized, blinded study. Our cohort was small, and we did not compare expert surgeons with novices. Participants were not randomized, and not all faculty members were blinded to the prior use of VR. There were also no initial evaluations before the course started, so it is not possible to measure improvement. As we mentioned before, the questionnaire used to assess participants needs to be validated, but it appears to be a good way of evaluating performance in the absence of measured metrics by the simulator.
Some of the potential benefits of the IVR are the possibility for widespread availability, portability, and a more accessible cost. This way residents and orthopedists could practice a surgical procedure many times with the actual instruments and implants; they will use in the operating room, even at home, or before a surgery without having to go to a skills lab. A combination of fracture skills courses and the availability of a VR simulator could be a good combination for learning the technique under supervision and then having the opportunity to practice until the whole technique is dominated before doing the actual procedure in the operating room.
We believe the next steps towards trauma-based IVR simulation research include larger randomized studies, internal and external validation studies, and establishing a method for determining proficiency. But most importantly, as we mentioned before, all of us, as physicians and surgeons, need to design training methods that involve learning, decision-making, and motor proficiency, incorporating all the technology that is quickly becoming available. We need to embrace the paradigm shift and realize that many aspects of surgical education need to be modified. It is not enough to have access to the latest technology and use a simulator to only develop motor skills. There needs to be a specific purpose in its use so that future development takes into account all these needs.
Finally, we think that the technological development in IVR simulation in orthopedic trauma should include: Better portability, haptic feedback, and complete immersion in the simulation (including sounds and other distractors, such as bleeding), specific metric measurements, and availability of many different procedures.
Conclusion
IVR simulation could be a more accessible way to provide a safe environment where participants can learn a new surgical technique. It is important to develop proficiency-based ptogressive training programs with specific educational goals that incorporate simulation and emerging technology as a tool. Larger, randomized, internal and external validation studies are needed.
Recommendations
IVR simulation with commercial hardware marks a new era in VR simulation, making it more accessible for most people and hospitals. This way, simulation can be more widely used to shorten the learning curve of specific and complex surgical techniques and implant application in orthopedic trauma. However, progressive training programs need to be developed incorporating this technology with a specific educational purpose and further development by the industry needs to be directed towards these goals.
Ethical consideration
All participants participated voluntarily and signed an informed consent.
Acknowledgements
We would like to thank all participants and faculty members who helped complete this research study. We would also like to thank the AO Trauma Mexico board for the support in doing this.
We would like to thank the Johnson and Johnson Institute for lending the VR simulators and extra Synbone® models.
Financial support and sponsorship
We did not receive any financial support from anyone to perform this study. However, the Johnson and Johnson Institute contributed with the VR simulators and ten proximal femur Synbone® models.
Conflict of interest
CAB is a consultant for Johnson and Johnson Medical, Mexico.
CAB, PJE, MAAC are members of AO Trauma and faculty members.
None of the other authors report a conflict of interest.
Author's contributions
CAB contributed with concepts, design, literature search, data acquisition and analysis, manuscript preparation, editing, and review. PJE contributed with concepts, design, data acquisition, editing, and review. MAAC contributed with data acquisition, editing, and review. JQF contributed with design, data analysis, editing, and review. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
| 1. | Stirling ER, Lewis TL, Ferran NA. Surgical skills simulation in trauma and orthopaedic training. J Orthop Surg Res 2014;9:126. [Google Scholar] |
| 2. | Camp CL, Krych AJ, Stuart MJ, Regnier TD, Mills KM, Turner NS. Improving resident performance in knee arthroscopy: A prospective value assessment of simulators and cadaveric skills laboratories. J Bone Joint Surg Am 2016;98:220-5. [Google Scholar] |
| 3. | Bartlett JD, Lawrence JE, Stewart ME, Nakano N, Khanduja V. Does virtual reality simulation have a role in training trauma and orthopaedic surgeons? Bone Joint J 2018;100-B: 559-65. [Google Scholar] |
| 4. | Guraya S. The changing landscape of surgical education and training. J Musculoskelet Surg Res 2018;2:1-3. [Google Scholar] |
| 5. | Atesok K, Satava RM, Marsh JL, Hurwitz SR. Measuring surgical skills in simulation-based training. J Am Acad Orthop Surg 2017;25:665-72. [Google Scholar] |
| 6. | Arroyo-Berezowsky C, Torres-Gómez A, Romo-Rodríguez R, Ruiz-Speare JO. Outcomes in virtual reality knee arthroscopy for residents and attending surgeons. J Musculoskelet Surg Res 2019;3:189-95. [Google Scholar] |
| 7. | Slade Shantz JA, Leiter JR, Gottschalk T, MacDonald PB. The internal validity of arthroscopic simulators and their effectiveness in arthroscopic education. Knee Surg Sports Traumatol Arthrosc 2014;22:33-40. [Google Scholar] |
| 8. | Egol KA, Phillips D, Vongbandith T, Szyld D, Strauss EJ. Do orthopaedic fracture skills courses improve resident performance? Injury 2015;46:547-51. [Google Scholar] |
| 9. | Sugand K, Mawkin M, Gupte C. Validating touch surgery™: A cognitive task simulation and rehearsal app for intramedullary femoral nailing. Injury 2015;46:2212-6. [Google Scholar] |
| 10. | Vaughan N, Dubey VN, Wainwright TW, Middleton RG. A review of virtual reality based training simulators for orthopaedic surgery. Med Eng Phys 2016;38:59-71. [Google Scholar] |
| 11. | Akhtar K, Sugand K, Sperrin M, Cobb J, Standfield N, Gupte C. Training safer orthopedic surgeons. Construct validation of a virtual-reality simulator for hip fracture surgery. Acta Orthop 2015;86:616-21. [Google Scholar] |
| 12. | van den Dobbelsteen JJ, Karahan M, Akguün U. Theory on psychomotor learning applied to arthroscopy. In: Karahan M, Kerkhoffs MM, Randelli P, Tuijthof JM, editors. Effective Training of Arthroscopic Skills. Berlin, Heidelberg: Springer Berlin Heidelberg; 2015. p. 17-32. [Google Scholar] |
| 13. | Nousiainen MT, McQueen SA, Hall J, Kraemer W, Ferguson P, Marsh JL, et al. Resident education in orthopaedic trauma: The future role of competency-based medical education. Bone Joint J 2016;98-B: 1320-5. [Google Scholar] |
| 14. | Luft HS, Bunker JP, Enthoven AC. Should operations be regionalized? The empirical relation between surgical volume and mortality 1979. Clin Orthop Relat Res 2007;457:3-9. [Google Scholar] |
| 15. | Bjorgul K, Novicoff WM, Saleh KJ. Learning curves in hip fracture surgery. Int Orthop 2011;35:113-9. [Google Scholar] |
| 16. | Gustafsson A, Pedersen P, Rømer TB, Viberg B, Palm H, Konge L. Hip-fracture osteosynthesis training: Exploring learning curves and setting proficiency standards. Acta Orthop 2019;90:348-53. [Google Scholar] |
| 17. | Seymour NE, Gallagher AG, Roman SA, O'Brien MK, Bansal VK, Andersen DK, et al. Virtual reality training improves operating room performance: Results of a randomized, double-blinded study. Ann Surg 2002;236:458-63. [Google Scholar] |
| 18. | Gallagher A. Proficiency-based progression simulation training for more than an interesting educational experience. J Musculoskelet Surg Res 2018;2:139-41. [Google Scholar] |
| 19. | Tay C, Khajuria A, Gupte C. Simulation training: A systematic review of simulation in arthroscopy and proposal of a new competency-based training framework. Int J Surg 2014;12:626-33. [Google Scholar] |
| 20. | The Osso Story. Osso VR; 2019. Available from: https://ossovr.com/the-osso-story/. [Last accessed on 2019 Aug 31, 20:53]. [Google Scholar] |
| 21. | Barad J. Personal Communication Through Linkedin Messaging With Just Barad MD, CEO Osso VR. Available from: https://www.linkedin.com ' justinbaradmd. [Last accessed on 2019 Sep 03]. [Google Scholar] |
Fulltext Views
5,887
PDF downloads
1,827




