
Translate this page into:
Wartenberg’s syndrome – A unique presentation resulting from compression of the superficial radial nerve from an anomalous radial artery branch

-
Received: ,
Accepted: ,
How to cite this article: Nijran A, Mirpuri L, Salibi A. Wartenberg’s syndrome – A unique presentation resulting from compression of the superficial radial nerve from an anomalous radial artery branch. J Musculoskelet Surg Res. doi: 10.25259/JMSR_9_2024
Abstract
Wartenberg’s syndrome is a compression sensorineural mononeuropathy of the superficial branch of the radial nerve. This case report describes a patient, who was severely debilitated by compression of the superficial branch of the radial nerve that she was unable to work. The case highlights a unique anatomical variation in the course of the deep terminal branch of the superficial radial artery causing compression of the superficial branch of the radial nerve. To the best of our knowledge, this has never been described before and should be considered a rare cause of Wartenberg’s syndrome. Surgery can provide both diagnostic and therapeutic benefits and should be considered early in such cases, especially when investigations are contradictory.
Keywords
Case report
Compression neuropathy
Radial artery
Radial nerve
Radial neuropathy
Wartenberg’s syndrome

INTRODUCTION
Wartenberg’s syndrome, named after the neurologist Robert Wartenberg, is a compression sensorineural mononeuropathy of the superficial branch of the radial nerve (SRN). This was previously known as cheiralgia paresthetica due to its similarities with compression of the lateral femoral cutaneous nerve, meralgia paresthetica.[1] The incidence rate of Wartenberg’s syndrome is unknown; however, the rate of radial nerve compressions generally is 0.003%.[2] It affects women four times more commonly than men.[2] Patients typically report pain, paresthesia, and numbness in the radial sensory nerve distribution, which supplies sensation to the dorsoradial aspect of the forearm and hand and also the dorsal aspect of the thumb, index, and middle fingers.[3] We present a case study of a unique anatomical variation of the radial artery’s deep terminal branch causing the SRN’s external compression.
CASE REPORT
A 36-year-old right-handed lady presented after a mechanical fall with severe pain over the first extensor compartment. Examination revealed no tenderness over the scaphoid and pain-free wrist movements. Plain radiographs revealed no wrist fractures, and she was initially thought to have De Quervain’s tenosynovitis and given an injection of 0.5% bupivacaine and 40 mg of triamcinolone and a wrist splint. The patient reported instant relief in symptoms. Four months later, the symptoms reoccurred with additional severe, debilitating wrist pain, worse on all wrist movements, and she also suffered from reduced sensation in the SRN distribution with reported 0/10 sensation in the index and middle fingers. She suffered from severe allodynia and was unable to work for over two years due to the pain. The patient described a throbbing nature to the pain. A further local anesthetic injection provided instant but temporary relief. An ultrasound scan revealed no tenosynovitis within the first extensor compartment, and nerve conduction studies revealed normal and symmetric sensory responses of the SRN. A magnetic resonance imaging of the wrist showed features of a prominent vessel in the anterolateral aspect of the wrist within the deep subcutaneous region, located in the region of the radial nerve, indicative of Wartenberg’s syndrome. A Duplex ultrasound suggested this vessel was a venous channel, possibly due to its aberrant nature. It did not behave like a normal artery on ultrasound.
The patient underwent surgical exploration, and the abnormal vessel identified was a branch of the radial artery traversing the SRN branches causing the patient’s symptoms [Figures 1 and 2]. This branch was ligated and removed resulting in complete relief of symptoms. The throbbing nature of the pain, which could not be explained at that time, in hindsight, may have been caused by the pulsation of the artery compressing the SRN. Six months post-surgery and after hand therapy for a stiff wrist, the patient was using her wrist and hand normally, with no allodynia. There was normal sensation over the thumb and index finger and slightly reduced sensation (7/10) over the dorsoradial hand. The patient had returned to work.
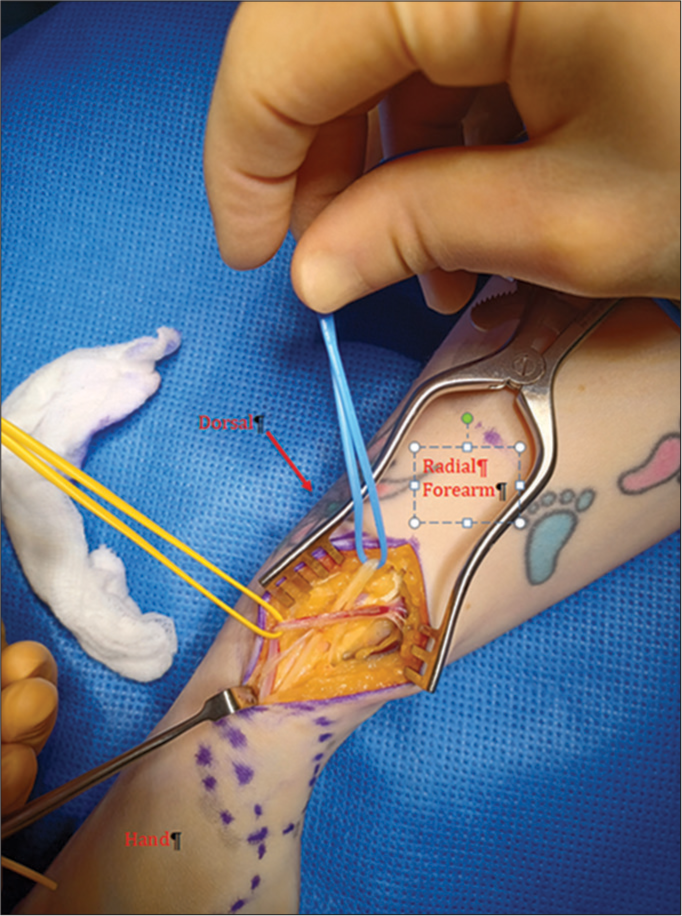
- Incision over radial aspect of forearm showing the anomalous radial artery traversing the branches of the superficial radial nerve.

- Superficial radial nerve shown in yellow with three branches being compressed by the aberrant dorsal radial nerve branch in red.
DISCUSSION
The SRN originates from the main radial nerve at the level of the lateral humeral epicondyle.[4] It pierces the deep fascia approximately 9 cm proximal to the radial styloid. It then bifurcates into two main branches approximately 5 cm proximal to the radial styloid before splitting into three further branches over the proximal dorsal wrist.[3]
Variations in the course of the radial artery have mainly been observed in the origin and proximal course rather than the distal course or terminal branches.[5] One anatomical study looking at 100 upper limb cadavers found no variation in the course of the radial artery. Furthermore, the radial artery was not closely related to other neurovascular structures in the forearm.[6] One study looking at the variation in the course of the radial artery found that a large palmar branch located radial and more superficial to flexor carpi radialis was most commonly encountered.[7] Extra-radial arteries result from disrupted embryologic development, which can also occur.[8] To the best of our knowledge, only one case report by Otsuka and Terauchi in 1991 describes an anomalous dorsal course of the radial artery. They identified a radial artery that went around Lister’s tubercle of the radius.[9] We present the first report of an anomalous distal deep branch of the radial artery, which had an unusual dorsal course before entering the anatomical snuffbox causing symptomatic acute compression of the SRN.
Peripheral neuropathies can be classified into acute traumatic crush injuries or chronic compression from inflammation, external compression or anatomic tether points.[3] Interestingly, this case was triggered by acute trauma resulting in the development of symptoms from a preexisting anatomic variation of the branch of the radial artery. The acute trauma may have precipitated an inflammatory response and swelling of the SRN resulting in the aberrant artery acting as a tether point.
The differential diagnoses for SRN entrapment include De Quervain’s intersection syndrome, radial styloid or scaphoid fractures, and cervical disc disease. De Quervain’s does not typically cause reduced sensation in the SRN distribution and does not give a typical Tinel’s sign. However, percussion over the first extensor compartment is likely to cause pain.[4] Furthermore, Finkelstein’s maneuver may be positive. Intersection syndrome classically presents with swelling and crepitus over the distal forearm with pain on resisted pronation.[10] Fractures of the radial styloid and scaphoid will typically be differentiated due to the mechanism, examination, and radiological findings. It is important also to rule out more proximal causes originating from the cervical spine.
CONCLUSION
This patient was severely debilitated by her symptoms, and the surgical release of the superficial radial nerve completely resolved her symptoms. In this case, the investigations were inconclusive and contradictory indicating the difficulty in diagnosing Wartenberg’s syndrome definitively. This case highlights a unique anatomical variation in the course of the superficial radial artery’s deep terminal branch causing SRN compression. To the best of our knowledge, this has never been described before and should be considered as a cause of Wartenberg’s syndrome. Early surgical exploration is advocated in such cases.
AUTHORS’ CONTRIBUTIONS
AS performed the surgical exploration and critically reviewed the draft and final manuscript. AN and LM wrote the manuscript. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
ETHICAL APPROVAL
The Institutional Review Board approval is not required.
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate patient consent forms. The patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published, and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
USE OF ARTIFICIAL INTELLIGENCE (AI)-ASSISTED TECHNOLOGY FOR MANUSCRIPT PREPARATION
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Uncommon upper extremity compression neuropathies. Hand Clin. 2013;29:443-53.
- [CrossRef] [PubMed] [Google Scholar]
- Split brachioradialis tendon causing Wartenberg syndrome in a professional baseball pitcher. J Hand Surg. 2023;5:239-41.
- [CrossRef] [PubMed] [Google Scholar]
- Part 5: compression neuropathies: Compression of the radial nerve In: Green's operative hand surgery (7th ed). Philadelphia, PA: Elsevier; 2017. p. :948.
- [Google Scholar]
- Clinically relevant variations in the origin and course of the radial artery. Anat Sci. 2021;18:7-14.
- [Google Scholar]
- Anatomical variations of the radial artery and its morphology with clinical implications. Int J Res Med Sci. 2022;10:2390-7.
- [CrossRef] [Google Scholar]
- Anatomic variations of the radial artery: Significance when harvesting for coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2004;127:1825-7.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of upper extremity ischemia In: Rutherford RB, ed. Vascular surgery (6th ed). Philadelphia, PA: Elsevier Saunders; 2005. p. :1274-93.
- [Google Scholar]
- An anomaly of the radial artery. Relevance for the forearm flap. Br J Plast Surg. 1991;44:390-1.
- [CrossRef] [PubMed] [Google Scholar]
- Intersection syndrome In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554494 [Last accessed on 2024 Jan 05]
- [Google Scholar]




