Translate this page into:
Huge finger
Corresponding Author:
Nizar A Al-Nakshabandi
Professor of Radiology, Department of Radiology, College of Medicine, King Saud University, Riyadh
Saudi Arabia
nizar97@hotmail.com
| How to cite this article: Al-Nakshabandi NA. Huge finger. J Musculoskelet Surg Res 2018;2:135-136 |
History
A 16-year-old asymptomatic boy with a large left hand and a swelling of the left index finger since birth.
- What are the findings?
- What is the differential diagnosis?
- What are the causes?
- What is the diagnosis?
Findings
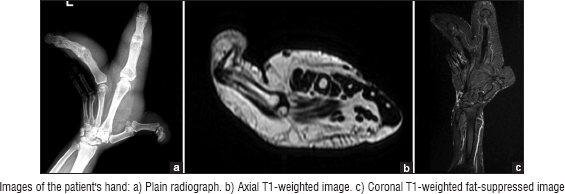
The anteroposterior hand plain radiograph (a) demonstrates macrodactyly and splaying of index and middle fingers with lengthened and broadened phalanges. There is an increased thickness soft tissue surrounding both digits. Interphalangeal joints of involved digits show narrowing and periarticular sclerosis, indicating degenerative changes. There is no osteophyte formation. Bone density is preserved otherwise.
Axial T1-weighted image (b) demonstrates macrodactyly and confirms the plain X-ray findings. Thickened soft tissue is hyperintense on T1, suggesting increased proliferation of subcutaneous fat. This abundant fat is not contained by a capsule. The signal intensity of abnormal fat is similar to that of subcutaneous fat. No focal lesion is seen. Phalanges of index and middle fingers are unremarkable, except the increased dimensions as compared to rest of the phalanges.
Coronal T1-weighted fat-suppressed image (c) demonstrates homogeneous saturation of the fat with no capsule. No focal tumor is seen. There is no evidence of lipofibromatous hamartoma of the median nerve.
Differential Diagnosis
- Macrodystrophia lipomatosa
- Fibromatous hamartoma of the nerves
- Neurofibromatosis Type I
- Vascular malformations (hemangioma or arteriovenous malformation)
- Hemihypertrophy
- Proteus syndrome.
Diagnosis
Macrodystrophia lipomatosa.
Pearls and Discussion
Macrodystrophia lipomatosa is a congenital condition. Loss of function and marked swelling of the affected limb or part of a limb is the most common presenting complaint.
On a pathological level, increased deposition of mesenchymal fat is seen with adipose tissue present in between the fibrous network which can involve the bone marrow, nerve sheaths, and muscles.
It could be associated with syndactyly (congenital fusion of 2 or more digits), clinodactyly (radial angulation of an interphalangeal joint at the radial ulnar or palmar planes), or polydactyly (more than the usual number of digits).
The condition is diagnosed with a plain radiograph which usually suffices. However, fat-saturated magnetic resonance imaging will help distinguish macrodystrophia lipomatosa from other differential diagnoses.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Further Reading
- Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ, et al. From the archives of the AFIP: Benign musculoskeletal lipomatous lesions. Radiographics 2004;24:1433-66.
- Khan RA, Wahab S, Ahmad I, Chana RS. Macrodystrophia lipomatosa: Four case reports. Ital J Pediatr 2010;36:69.
- Abdulhady H, El-Sobky TA, Elsayed NS, Sakr HM. Clinical and imaging features of pedal macrodystrophia lipomatosa in two children with differential diagnosis review. J Musculoskelet Surg Res 2018;2:130-4.
Fulltext Views
2,566
PDF downloads
2,162




