Translate this page into:
Acute knee trauma after anterior cruciate ligament reconstruction
Corresponding Author:
Nizar A Al-Nakshab
Department of Radiology, King Saud University, Riyadh
Saudi Arabia
nizar97@hotmail.com
| How to cite this article: Al-Nakshab NA. Acute knee trauma after anterior cruciate ligament reconstruction. J Musculoskelet Surg Res 2019;3:237-238 |
History
A 25-year-old male football player had previous reconstruction of the anterior cruciate ligament (ACL) presented after acute knee trauma while playing football. Physical examination shows an equivocal Lachman and pivot shift test.
- What are your findings?
- What is the differential diagnosis?
- What are the causes?
Findings
Coronal T2-weighted images with fat saturation [Figure - 1]a demonstrate bone contusion in the medial tibial condyle presenting as high-signal intensity.
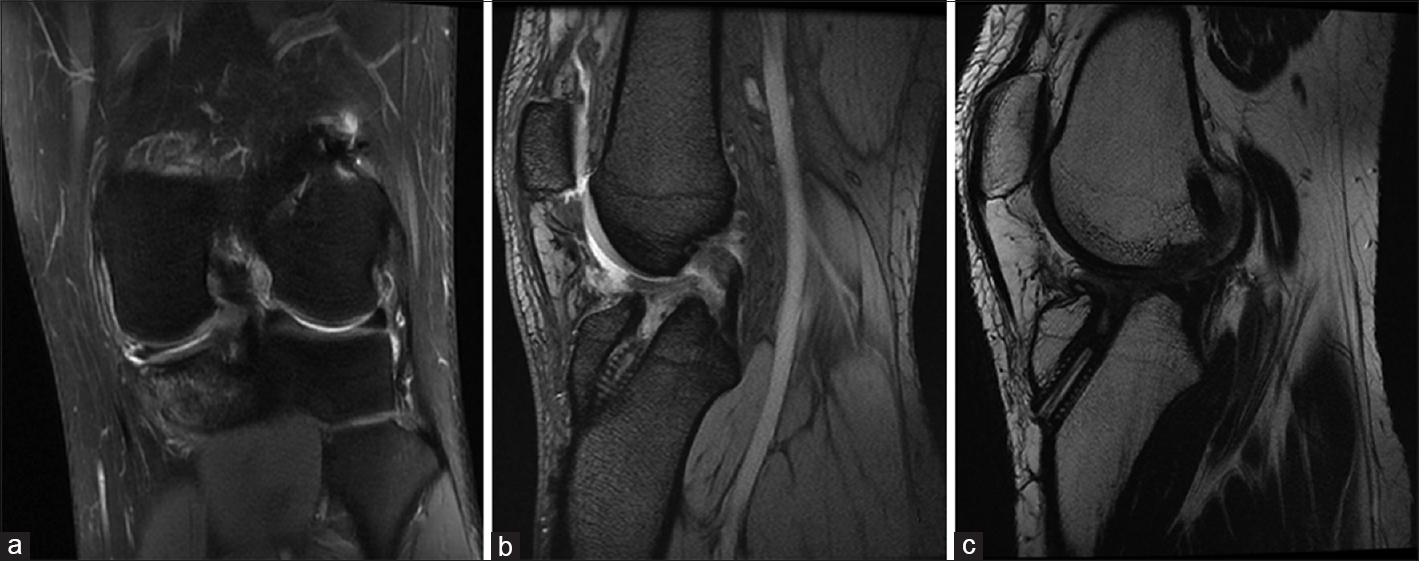 |
| Figure 1 |
Sagittal oblique gradient echo images [Figure - 1]b and T1 [Figure - 1]c demonstrate fiber discontinuity of the ACL graft. The ACL angle is no longer parallel to Blumensaat's line.
Diagnosis
ACL graft tear.
Pearls and Discussion
Signs of ACL graft tears could be divided into primary and secondary signs. The primary signs are swelling, fiber discontinuity, and change in the course of the ACL where the ACL angle is no longer parallel to Blumensaat's line. Other signs as in our case here is bone contusion, more than 7 mm of anterior tibial translation, look for other signs such as Segond fracture, and buckling of the posterior cruciate ligament (PCL).
The O'Donoghue unhappy triad constitutes tear of the ACL, tear of the medial collateral ligament, and medial meniscal tear.
A triad has been revisited considered surgical findings where lateral meniscal injury is more common than injury to the medial meniscus. This makes more sense from a biomechanical point of view.
On plain radiographs, look for the deep sulcus sign, anterior tibial translation sign, Segond fracture, and arcuate fracture or joint effusion were noted.
Magnetic resonance imaging (MRI) is critical in the evaluation of the postoperative knee, and the ACL reconstruction patient is no exception. Common indications for utilizing MRI in the postoperative ACL patient include acute reinjury, persistent instability, limitation of motion, or simply persistent pain. In cases of acute reinjury, such as the current example, MRI often directly visualizes the edema and laxity of a recurrent tear. In cases where a graft tear is poorly visualized, any of the secondary signs of ACL disruption such as pivot shift, bone bruises, or PCL buckling may also be utilized in the ACL graft patient. As with native ACL injuries, MRI allows evaluation of associated meniscal, chondral, or osseous abnormalities in patients who have suffered an ACL graft tear. Caution should be used when evaluating a failed ACL graft with MRI, as it may be unreliable and inconsistent. Disruption of the reconstructed ligament on MRI should be combined with a concordant clinical examination and a clear medical history of a new trauma. MRI evaluation could sometimes be misleading because of the discordance between clinical examination and MRI evaluation.
Therefore, it is possible to see an apparently normal graft on MRI but clinically or arthroscopically injured or elongated.
MRI should be considered an additional and not exclusive tool for the assessment of the post-operative ACL. It is well known that the inter- and intra-observer reliability for the MRI evaluation of the ACL graft is moderate. Sensitivity and specificity of MRI to detect an ACL graft tear in some studies was only 60% and 80%, respectively.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Further Reading
- Sanders TG, Medynski MA, Feller JF, Lawhorn KW. Bone contusion patterns of the knee at MR imaging: Footprint of the mechanism of injury. Radiographics 2000;20:S135-51.
- Shelbourne KD, Nitz PA. The O'donoghue triad revisited. Combined knee injuries involving anterior cruciate and medial collateral ligament tears. Am J Sports Med 1991;19:474-7.
- O'donoghue DH. Surgical treatment of fresh injuries to the major ligaments of the knee. J Bone Joint Surg Am 1950;32 A: 721-38.
Fulltext Views
4,438
PDF downloads
1,990





![[Figure - 1]](#fig_SaudiOrthopJ_2019_3_2_237_249268_f1.jpg){kind=link}