
Translate this page into:
Low- versus high-dose botulinum toxin A injection for the treatment of upper limb spasticity in pediatric patients with cerebral palsy: A systematic review and meta-analysis
*Corresponding author: Lama Alqarni, Medical Intern, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia. Lamaalq17@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bamaga AK, Alqarni L, Awami HM, Alazwari HF, Almehmadi SM, Aldharrab AS. Low- versus high-dose botulinum toxin type A injection for the treatment of upper limb spasticity in pediatric patients with cerebral palsy: A systematic review and meta-analysis. J Musculoskelet Surg Res. 2025;9:4-10. doi: 10.25259/JMSR_196_2024
Abstract
Botulinum toxin type A (BTX-A) is widely used for pain control and muscle spasticity management. In children with spastic predominant cerebral palsy (CP), direct BTX-A injection into muscle can temporarily reduce spasticity. This study aimed to compare the safety and efficacy of BTX-A injections administered at high and low doses in reducing upper limb spasticity in CP children. This is a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing low-dose (2–6 U/kg) and high-dose (8–16 U/kg) BTX-A injections using a computerized search in MEDLINE, Web of Science, Google Scholar, mRCT, and Clinicaltrials. gov without restriction on language or data from the database inception to August 24, 2023. The following terms were used: “Cerebral Palsy” AND “Upper Extremity OR Upper Limb” AND “Botox Injection OR Botulinum Toxin Type A.” The inclusion criteria were RCTs that compared BTX-A injection doses and measured the efficacy and safety of doses on the upper extremities of children with CP. The primary outcomes were the modified Ashworth scale (MAS), goal attainment scaling (GAS), and adverse events (AEs). The risk of bias assessment was performed using the revised Cochrane risk of bias assessment tool. Three RCTs with 512 participants met the inclusion criteria. There are no significant differences in terms of MAS, GAS or AEs between the high-dose and low-dose BTX-A. There were no significant differences in efficacy or AEs between high-dose and low-dose BTX-A used in the upper extremities of children with CP. Further research on long-term outcomes and functional benefits is warranted.
Keywords
Botulinum toxins type A
Cerebral palsy
Muscle spasticity
Pediatrics
Upper extremities

INTRODUCTION
Cerebral palsy (CP) is a lifelong neurological condition that affects posture, mobility, and muscle tone. CP presents in three main forms: Spastic type, dyskinetic type, and ataxic and mixed type.[1] Among these, the spastic type reigns dominant, impacting around 80% of children with CP.[2-4]
Spastic CPs’ clinical appearance varies widely, depending on the location and time the brain injury occurred.[5] While both upper and lower motor neurons can be affected, damage to the upper motor neuron often holds the reins, significantly hindering daily life functions. For pediatric neurologists, tackling this disability takes center stage, leading them to prioritize management options for this specific type of CP. The mainstay of treatment is occupational therapy, physiotherapy, and anti-spastic pharmacotherapy.[6]
By inhibiting the presynaptic production of acetylcholine from motor endplates of the lower motor nerve at the myoneural junction, Botulinum toxin A (BTX-A) injections directly into the muscle can temporarily reduce spasticity in children with spastic predominating CP.[6]
The first paper that used BTX-A in children with CP was by Koman et al. in the United States in 1993. The study was conducted on 27 children with CP, and the conclusion indicated that BTX-A injection is a safe method that can improve muscle spasticity and delay surgical interventions.[7]
In a double-blind, randomized, and placebo-controlled study, Corry et al. found that giving injections to several muscles in the spastic upper extremity of children with CP may improve their tone, range of motion, grasp, and cosmesis. Still, they did not affect their functional ability when picking up coins.[8]
Despite its established role, the optimal BTX-A dosage remains an ongoing investigation. While some studies advocate for higher doses (8–16 U/kg) for their superior spasticity reduction compared to lower ones (2–6 U/kg), others paint a different picture. Studies indicate that the dosage could not substantially affect upper extremity function as determined by certain assessments such as the Quality of Upper Extremity Skills Test (QUEST). Adding to the complexity, other studies indicate efficacy across all dose ranges (2 U/kg, 6 U/kg, and 8 U/kg) for different clinical patterns of spasticity. Compared to the low dosage 2 U/kg control, therapy with 8 U/kg or 16 U/kg BTX-A in the afflicted upper limb dramatically improved muscular tone and spasticity in one randomized trial.[9]
Furthermore, a three-month study using the QUEST to compare the dosage of BTX-A in the upper extremities of children with spasticity found no statistically significant difference in upper extremity function between the low-dose and high-dose groups.[10,11]
In addition, according to another randomized controlled trial (RCT),[12] all three dosages (8 U/kg, 6 U/kg, and 2 U/kg) substantially decreased spasticity in all three dose groups across all upper-limb clinical characteristics treated.
Navigating this sea of conflicting findings can be daunting for clinicians, caregivers, and patients. This is where our systematic review steps in. To manage spasticity and enhance upper limb mobility and function in children with CP, we aimed to thoroughly examine research on low-dose versus high-dose BTX-A injections. By weighing each approach’s benefits and potential side effects, we hope to equip health-care professionals and families with evidence-based information to guide their decision-making process and pave the way for optimizing spasticity management in this vulnerable population.
MATERIALS AND METHODS
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis checklist was applied to perform and document this study using a specified methodology.
Eligibility criteria
RCT studies examining the effects of BTX-A at high and low doses on upper limb function in patients under 18 with CP met the review’s inclusion requirements. We aimed to assess the following outcomes: Modified Ashworth scale (MAS),[13] Goal Attainment Scaling (GAS),[14] and Adverse Events (AEs). Studies using non-human subjects or in vitro research, duplicates or overlaps, articles having abstracts only as predecessor papers, conference proceedings, editorials, author response theses, and books were all eliminated. We also did not include case reports, case series, systematic review studies, and papers for which the entire text is inaccessible.
Search strategy
The systematic search was applied using MEDLINE, Web of Science, Google Scholar, mRCT, and Clinicaltrials.gov without restriction on language or data from the database inception to August 24, 2023. We used the following terms in searching throughout the databases: CP AND (Upper Extremity OR Upper Limb) AND (Botox Injection OR BTX-A). We also reviewed the reference lists of the included RCTs to find possibly relevant RCTs that were overlooked during the systematic search.
Study selection and data extraction
Data extraction from eligible trials, full-text evaluation, and eligibility screening of titles and abstracts were all carried out separately and duplicated by two reviewers. A third reviewer’s judgment was used to resolve disagreements.
Meta-analysis
The data analysis used Review Manager version 5.4 (Cochrane Collaboration). Every statistical evaluation followed the random-effects model. Statistical significance was defined as P < 0.05 and a 95% confidence level. I2 and the P-value of the Chi-squared test for heterogeneity were used to evaluate the statistical heterogeneities. The standardized mean difference was chosen for continuous findings, whereas the odds ratio (OR) was applied for dichotomous results.
Risk of bias assessment
Two authors evaluated the possibility of bias for the eligible RCTs individually and in duplicate, applying the revised Cochrane risk of bias assessment tool. We used symmetry analysis and a visual examination of the funnel plot to evaluate the possibility of publishing bias.
RESULTS
Search
Our comprehensive search through 584 articles yielded only three eligible RCTs on BTX-A dosage for children with CP with upper limb spasticity [Figure 1].[9,11,12]
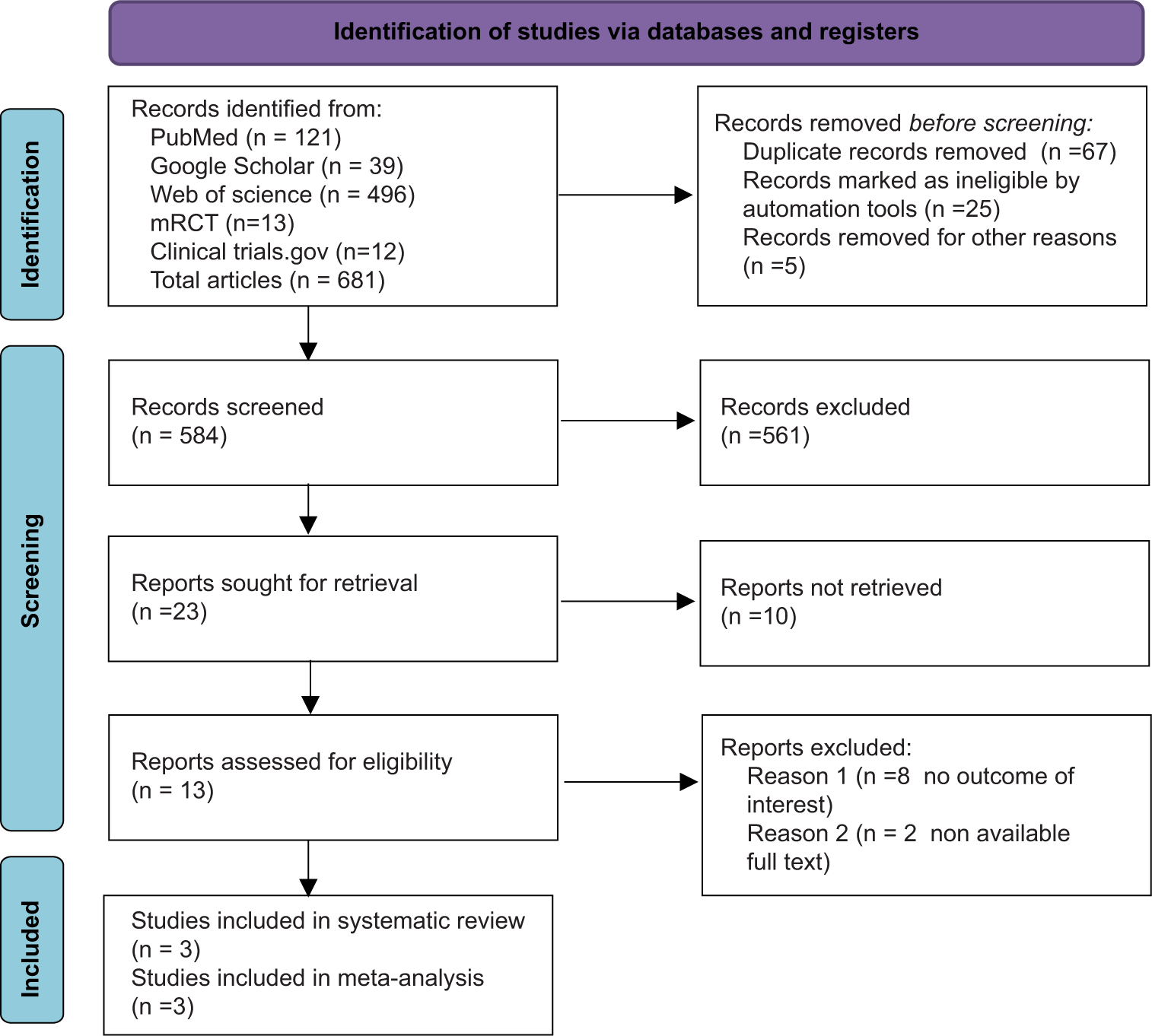
- Flow diagram.
Trial characteristics
Studies published between 2007 and 2021 involved 512 participants averaging 4–9 years old. Of these, 337 received high-dose BTX-A, and 175 received low-dose, with a roughly two-thirds to one-third ratio [Table 1].
| Study characteristics | ||||||||
|---|---|---|---|---|---|---|---|---|
| Study, Year | Study participants | Randomization | Doses | Sex, M:F | Bilateral CP included | Mean age (Years) | Time of Follow-up | Measured outcomes |
| Dabrowski et al., 2021[12] | 263 | Low dose: 87 High dose: 176 |
Low dose: 2 U/kg/limb High dose: 8 U/kg/limb |
220:130 | Yes | Low dose: 7.2 High dose: 7.3 |
14 weeks±2 weeks | MAS GMFCS AE |
| Delgado et al., 2020[9] | 84 | Low dose: 70 High dose: 140 |
Low dose: 2 U/kg/limb High dose: 8 U/kg and 16 U/kg/limb |
126:84 | Yes | Low dose: 9 High dose: 9.2 |
Baseline, at week 6 and week 16 | MAS GAS PGA MTS TEAE |
| Kawamura et al., 2007[11] | 39 | Low dose: 18 High dose: 21 |
Low dose: Maximum of 25U/site High dose: Maximum of 50U/site |
22:17 | Yes | Low dose: 3.1 High dose: 2.6 |
Baseline, at 1 month and 3 months | QUEST PEDI MAS GAS Grip strength AE |
CP: Cerebral palsy, MAS: Modified Ashworth scale, GMFCS: Gross motor function classification system, AE: Adverse events, GAS: Goal attainment scaling, PGA: Physician global assessment, MTS: Modified Tardieu scale, TEAE: Treatment-emergent adverse events, QUEST: Quality of upper extremity skills test, PEDI: Pediatric evaluation of disability inventory
Risk of bias assessment
Two of the three included RCTs were considered to have a low overall risk of bias, while one’s missing outcome data raised a few concerns. None of the studies showed any evidence of a significant overall risk of bias [Figures 2 and 3].
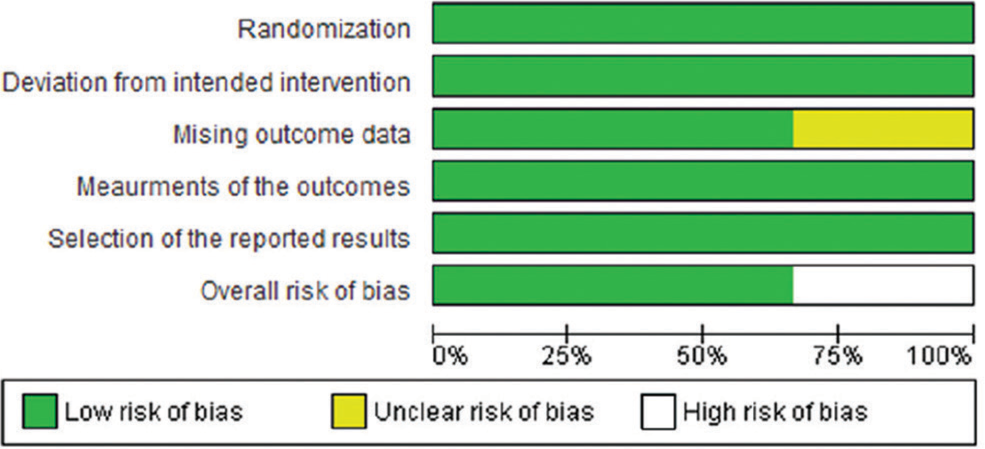
- Risk of bias graph.
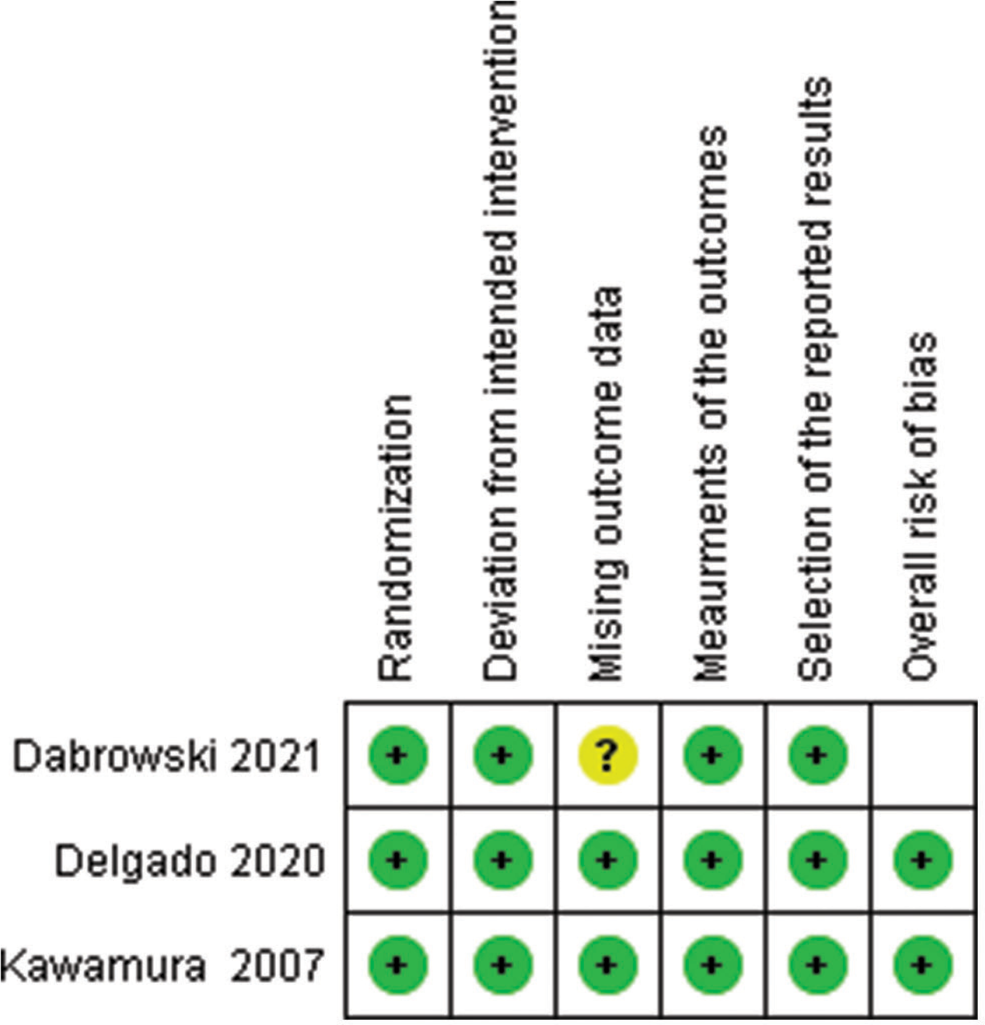
- Risk of bias summary. Yellow circle (question mark): Unclear risk of bias, green circle (plus sign): Low risk of bias, empty box: High risk of bias.
Outcomes
GAS
Two RCTs provide data about GAS.[9,11] A total of 53 individuals were allocated low doses of BTX-A, and 66 were allocated high doses of BTX-A. Data were reported at follow-up periods of 3 months. Overall, there was no apparent difference between the high and low doses in terms of GAS (standard deviation mean [SDM] = 0.11, 95% confidence interval [CI] [–0.25, 0.48], with P-value of = 0.54) [Figure 4]. Since the funnel plot was symmetric, there was no evidence of publishing bias.

- Forest plot for Goal Attainment Scaling after 3 months of Botulinum toxin type A injection. SD: Standard deviation, IV: Weighted mean difference, CI: Confidence interval, df: Degrees of freedom, Chi2: Chi-square statistic, P: P-value, I2: I-square heterogeneity statistic, Z: Z statistic.
MAS
All three RCTs provided data about the MAS.[9,11,12] A total of 175 individuals were allocated low doses of BTX-A, and 265 were allocated high doses of BTX-A. Data were reported by muscle groups. Overall, low dosage and high dose did not significantly differ from one another in terms of MAS (SDM = −0.01, 95% CI [–0.21, 0.19], with a P-value of = 0.93) [Figure 5]. The funnel plot was asymmetric, which indicates that there is a notable publication bias.

- Forest plot for Modified Ashworth scale after Botulinum toxin type A injection. SD: Standard deviation, IV: Weighted mean difference, CI: Confidence interval, df: Degrees of freedom, Chi2: Chi-square statistic, P: P-value, I2: I-square heterogeneity statistic, Z: Z statistic.
AEs
All three RCTs provided data about the AEs.[9,11,12] Overall, there was no discernible difference between the high and low dosages (OR = 1.12, 95% CI [0.77, 1.62], with a P-value of = 0.55) [Figure 6]. The funnel plot was asymmetric, indicating a notable publication bias.
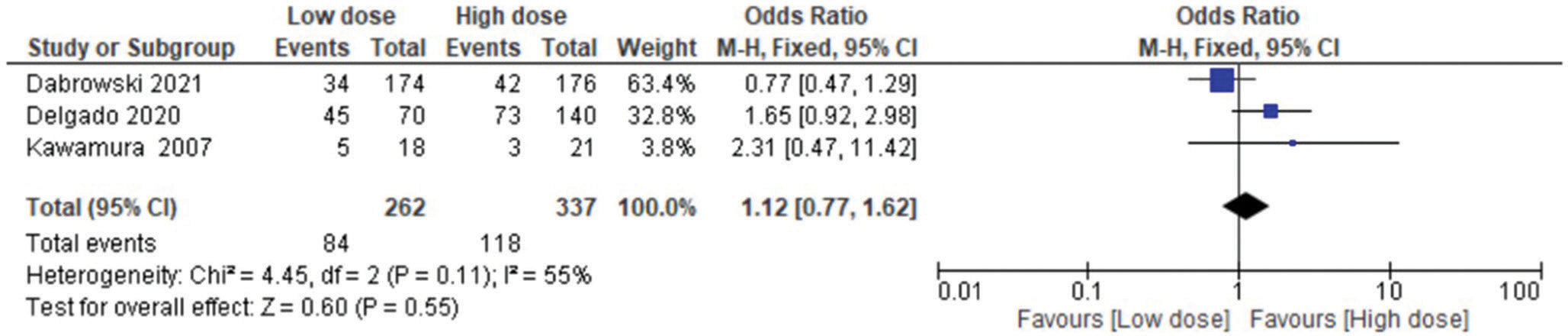
- Forest plot for intensity of the adverse events after botulinum toxin type A injection. M-H: Mantel-Haenszel, CI: Confidence interval, df: Degrees of freedom, Chi2: Chi-square statistic, P: P-value, I2: I-square heterogeneity statistic, Z: Z statistic.
DISCUSSION
The results of this systematic review and meta-analysis, encompassing three RCTs with 512 participants, aimed to compare the efficacy of high-dose (8–16 U/kg) versus low-dose (2–6 U/kg) BTX-A injections in enhancing upper limb mobility and function in pediatric CP patients.
BTX-A functions by inhibiting acetylcholine release at the neuromuscular junction, reducing muscle spasticity and improving motor function. This mechanism is particularly beneficial for managing spasticity in children with CP, as it allows for temporary muscle relaxation, facilitating better movement and potentially enhancing the effectiveness of adjunct therapies such as physiotherapy and occupational therapy.[6]
Our findings indicate that in terms of functional outcomes assessed using the GAS, there was no significant difference between low-dose and high-dose BTX-A injections. This result suggests that both dosage regimens might provide similar benefits in reaching specific functional goals. Similarly, assessments using the MAS did not show a significant difference between the two dosage groups, indicating similar reductions in muscle tone irrespective of BTX-A dosage. These results align with the previous studies that have failed to demonstrate a clear superiority of high-dose over low-dose BTX-A injections in improving upper limb spasticity.[11]
It is also essential to note that the incidence of adverse effects did not change significantly between the BTX-A groups receiving high and low doses. The comparable safety profiles of both dosing regimens assure physicians of the relative risk of BTX-A injections in children with CP. This is particularly important as safety is a critical consideration in pediatric treatments.
A recent evidence-based review corroborated that BTX-A injections could improve body function and activity alongside reducing spasticity as measured by MAS.[15] Moreover, a systematic review supports the idea that using BTX-A injections on the upper limbs of children with CP can yield good outcomes by reducing spasticity. However, the review also emphasized that BTX-A should be combined with occupational or physiotherapy to achieve optimal results. This same study reported that the safe dose with minimal side effects ranged from 0.5 U to 16 U/kg body weight.[6]
Regarding the effect of BTX-A injections in the lower extremities of children with CP, both low and high doses were associated with improvements in the passive range of motion as measured by the Tardieu scale. In addition, higher doses were found to be safe and well-tolerated, similar to our findings for upper limb treatments.[16]
In addition to treating spasticity in CP, BTX-A has several other medical indications. These include managing chronic migraines, treating hyperhidrosis (excessive sweating), addressing overactive bladder, and reducing the appearance of facial wrinkles.[17-20] BTX-A is also used in the treatment of conditions such as cervical dystonia, blepharospasm (uncontrolled blinking), and strabismus (crossed eyes), highlighting its versatility and broad therapeutic potential.[21]
Finally, the distinction between upper and lower limb spasticity is significant. Lower limb spasticity often involves more widespread and severe spasticity, which might require higher doses of BTX-A, while upper limb spasticity typically requires a more precise, individualized dosing approach. Although further research is necessary, there is potential for the higher doses used to treat lower limb spasticity to be applied to upper limb spasticity, potentially improving outcomes in some cases.
In conclusion, our findings suggest that both low-dose and high-dose BTX-A regimens offer comparable efficacy and safety profiles in managing upper limb spasticity in children with CP. Therefore, factors such as patient tolerance, injection site concerns, and recent treatment outcomes should be considered when choosing a dosing strategy. Moreover, it is important to consider in future studies that higher doses involve greater costs, and as indicated in this paper, higher doses do not necessarily result in better outcomes. This economic consideration is crucial for both health-care providers and patients’ families when planning long-term management strategies for CP. On the other hand, from a long-term perspective, higher doses may prove more cost-effective, as they typically require fewer sessions per year. Furthermore, the higher dose group often experiences a longer sustained duration of improvement compared to the lower dose group, which can alleviate emotional distress for the child and reduce interruptions to family life.[6]
Strengths
This meta-analysis boasts several notable strengths. This is the first meta-analysis that we are aware of. We tried to minimize the possibility of confounding variables using strict exclusion criteria. To provide a more homogeneous participant group, the patient population chosen for this study particularly included those with CP. The comprehensive assessment of the selected RCTs with the Cochrane risk of bias instrument (RoB-2),[22] which enabled us to pinpoint gaps in the existing body of evidence and suggest future lines of inquiry, lends additional support to our study. Furthermore, the most reliable tools for evaluating upper limb function were used to analyze the effectiveness of both doses.
Limitations
Several factors necessitate a cautious interpretation of our findings. First, with only three included RCTs, our review has limited generalizability. In addition, participant variation across studies potentially impacted statistical power. Furthermore, while we categorized BTX-A doses as low and high, slight deviations in their definitions across studies may hinder result comparability.
Next, the included RCTs’ use of diverse outcome measures might introduce inconsistencies in evaluating treatment effects. Moreover, disparities in muscle localization techniques across studies could compromise data interpretation. Finally, the relatively short follow-up periods of 1 and 3 months limit our understanding of long-term BTX-A dose effects in children with CP.
Taking into account that various muscle groups were targeted for injection in the studies is also crucial. Commonly treated upper limb muscles included the biceps brachii, triceps brachii, and the flexor and extensor muscles of the forearm. The doses used in practice typically range from 2 to 10 U per muscle, depending on factors such as muscle size and spasticity severity. This variability in muscle targeting and dosing could influence treatment outcomes and should be considered when interpreting. In addition, we could not differentiate between types of CP among the participants in our review. Different CP types, such as dystonic CP, might require different BTX-A dosages to achieve the best possible outcomes due to variations in muscle spasticity.
CONCLUSION
This study provides valuable clinical insights. We have demonstrated that high-dose and low-dose BTX-A did not differ significantly in efficacy or AEs regarding the outcomes we assisted in this review. However, further research is crucial.
RECOMMENDATIONS
Future trials should include larger sample size, longer follow-ups, consistent dose definitions, and comprehensive safety assessments to optimize BTX-A therapy while avoiding adverse effects. Nevertheless, considering the possible limitations, we suggest caution when using this finding.
AUTHORS’ CONTRIBUTIONS
AKB contributed to the study’s design and writing of the final manuscript. LA contributed to the research idea, design of the study, data extraction, statistical analysis/interpretation, risk of bias assessment, and editing of the final manuscript. HMA and HFA contributed to the study’s design, data extraction, risk of bias assessment, and final manuscript writing. SMA and ASA contributed to the data extraction and writing of the final manuscript. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
ETHICAL APPROVAL
The Institutional Review Board approval is not required.
DECLARATION OF PATIENT CONSENT
Patient’s consent was not required as there are no patients in this study.
USE OF ARTIFICIAL INTELLIGENCE (AI)-ASSISTED TECHNOLOGY FOR MANUSCRIPT PREPARATION
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- A report: The definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007;109:8-14.
- [Google Scholar]
- Cerebral palsy in children: An overview. J Clin Orthop Trauma. 2012;3:77-81.
- [CrossRef] [PubMed] [Google Scholar]
- Cerebral palsy in Victoria: Motor types, topography and gross motor function. J Paediatr Child Health. 2005;41:479-83.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical spectrum, comorbidities, and risk factor profile of cerebral palsy children: A prospective study. J Pediatr Neurosci. 2017;12:15-8.
- [CrossRef] [PubMed] [Google Scholar]
- Identification and measurement of dystonia in cerebral palsy. Dev Med Child Neurol. 2017;59:1249-55.
- [CrossRef] [PubMed] [Google Scholar]
- Botulinum toxin A as an adjunct to treatment in the management of the upper limb in children with spastic cerebral palsy (UPDATE) Cochrane Database Syst Rev. 2010;2010:CD003469.
- [CrossRef] [PubMed] [Google Scholar]
- Management of cerebral palsy with botulinum-A toxin: Preliminary investigation. J Pediatr Orthop. 1993;13:489-95.
- [CrossRef] [PubMed] [Google Scholar]
- Botulinum toxin A in the hemiplegic upper limb: A double-blind trial. Dev Med Child Neurol. 1997;39:185-93.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy and safety of abobotulinumtoxinA for upper limb spasticity in children with cerebral palsy: A randomized repeat-treatment study. Dev Med Child Neurol. 2021;63:592-600.
- [CrossRef] [PubMed] [Google Scholar]
- Quality of upper extremity skills test Hamilton, Ontario: McMaster University, Clinical Research Unit; 1992.
- [Google Scholar]
- A randomized controlled trial comparing botulinum toxin A dosage in the upper extremity of children with spasticity. Dev Med Child Neurol. 2007;49:331-7.
- [CrossRef] [PubMed] [Google Scholar]
- IncobotulinumtoxinA efficacy/safety in upper-limb spasticity in pediatric cerebral palsy: Randomized controlled trial. Pediatr Neurol. 2021;123:10-20.
- [CrossRef] [PubMed] [Google Scholar]
- Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987;67:206-7.
- [CrossRef] [PubMed] [Google Scholar]
- Goal Attainment Scaling (GAS) in rehabilitation: A practical guide. Clin Rehabil. 2009;23:362-70.
- [CrossRef] [PubMed] [Google Scholar]
- Safety and efficacy of botulinum toxin type A preparations in cerebral palsy-an evidence-based review. Neurol Neurochir Pol. 2021;55:158-64.
- [CrossRef] [PubMed] [Google Scholar]
- High dose botulinum toxin A for the treatment of lower extremity hypertonicity in children with cerebral palsy. Dev Med Child Neurol. 2007;49:818-22.
- [CrossRef] [PubMed] [Google Scholar]
- Nonpharmacologic treatments for chronic and episodic migraine: A systematic review and meta-analysis. Plast Reconstr Surg. 2023;152:1087-98.
- [CrossRef] [PubMed] [Google Scholar]
- Botulinum toxin A and B for palmoplantar hyperhidrosis. Dermatol Ther (Heidelb). 2024;14:805-11.
- [CrossRef] [PubMed] [Google Scholar]
- The use of botulinum toxin in various urological conditions. Wiad Lek. 2024;77:348-52.
- [CrossRef] [PubMed] [Google Scholar]
- Botulinum neurotoxin serotype A: A clinical update on non-cosmetic uses. Am J Health Syst Pharm. 2004;61:S11-23.
- [CrossRef] [PubMed] [Google Scholar]
- RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
- [CrossRef] [PubMed] [Google Scholar]




