
Translate this page into:
Bilateral triceps and unilateral quadriceps tendon rupture in a patient with end-stage renal disease: A case report and review of literature
*Corresponding author: Dr. Rahaf Bashaweeh, Department of Orthopedics Surgery, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia. rahafbashweh@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bashaweeh R, Alhumaid I, Makhdoum A, Alraiyes T. Bilateral triceps and unilateral quadriceps tendon rupture in a patient with end-stage renal disease: A case report and review of literature. J Musculoskelet Surg Res. 2025;9:271-5. doi: 10.25259/JMSR_367_2024
Abstract
Spontaneous tendon rupture is a rare complication of chronic metabolic diseases. We report a rare case of a simultaneous bilateral triceps and unilateral quadriceps tendon rupture in a 22-year-old male, who is known to have chronic kidney disease and is on long-term hemodialysis. He presented to our hospital after a history of a simple fall. Our management consisted of surgical repair of all ruptured tendons in one setting. To our knowledge, no cases of bilateral triceps and unilateral quadriceps tendon rupture in the same patient have been reported in the literature thus far. Overall, spontaneous tendon rupture is a rare occurrence. In literature, management of such cases has been reported to be treated surgically. In this case report, we discuss the diagnosis and operative treatment and highlight how early surgical intervention is a key factor in the rehabilitation and functional outcome of the patient.
Keywords
Quadriceps tendon
Renal failure
Tendon repair
Tendon rupture
Triceps tendon

INTRODUCTION
Spontaneous tendon rupture in chronic metabolic diseases is considered a rare complication.[1] In end-stage renal disease, the consequences of chronic hemodialysis can lead to the degeneration of tendons and ligaments, which in turn can lead to spontaneous rupture.[2] A few cases of quadriceps and triceps tendon rupture have been reported in the literature. Management consists of early surgical repair as it leads to fewer complications and better outcomes.[3,4] The most common cause of tendon rupture, in general, is trauma. Spontaneous tendon ruptures, however, are rare and multifactorial. They are mostly associated with long-term hemodialysis. Achilles tendon, quadriceps tendon, and rotator cuff tendons are reported to be the most common to rupture. The largest number of groups reported was 16 tendons in nine patients with end-stage renal disease.[1] Here, we discuss an interesting case of bilateral triceps tendon rupture associated with unilateral quadriceps tendon rupture in a patient with chronic renal disease and review the literature. The pathogenesis, diagnosis, and management of these challenging injuries in these patient populations will be discussed further in this study.
CASE REPORT
We report a 22-year-old young man, who presented to us with an acute episode of bilateral elbows and right knee pain with limitation of motion after sustaining minor trauma caused by falling on his right knee when he suddenly tripped on a solid object at home while holding walls with both hands. He could not bear weight after the fall. He is a known case of end-stage renal disease due to primary focal segmental glomerulosclerosis, had received regular hemodialysis for four years, and is following in our hospital for a pre-transplant workup. He also has hypertension, normocytic anemia, and secondary hyperparathyroidism. He is taking only bisoprolol, sevelamer, and cinacalcet, and he does not have a history of smoking or drinking. He is right-hand and lower-limb dominant and does not have a similar history of presenting symptoms. Pre-injury, the patient was an independent mobilizer without functional disabilities in both upper and lower limbs. He had a full range of motion (ROM) in his elbows and knees.
A physical examination of his right knee demonstrated tender suprapatellar swelling with palpable defect, disrupted extensor mechanism, and inability to do active knee extension. Examination of his elbows showed moderate swelling and tenderness around the olecranon, with limited active extension against gravity (could do 20–30° only) bilaterally. Initial radiographic evaluation revealed right knee effusion along with soft-tissue swelling and osseous avulsion of quadriceps tendon with retraction, bilateral elbow effusion, fat pad sign with soft-tissue swelling along olecranon process, and calcification over distal triceps, which are more obvious on the right side. Further assessment with computed tomography and magnetic resonance imaging (MRI) scans confirmed the findings. There was a 1.2 cm gap between the patella and retracted quadriceps tendon with completely torn medial and lateral retinacular attachments from the patella, along with a calcified tendinous stump and signs of chronic tendinosis. Similarly, there were full-thickness tears of tricep tendons with gaps of 0.7 and 1.7 cm on the right and left side, respectively, along with calcified tendon stumps and features of chronic tendinosis [Figures 1 and 2].

- (a) Radiograph of the right knee with obvious effusion and osseous avulsion of the quadriceps tendon, (b) Computed tomography scan, sagittal cut. (c and d) Are magnetic resonance imaging sagittal and coronal cuts clearly identify complete avulsion of the quadriceps tendon.
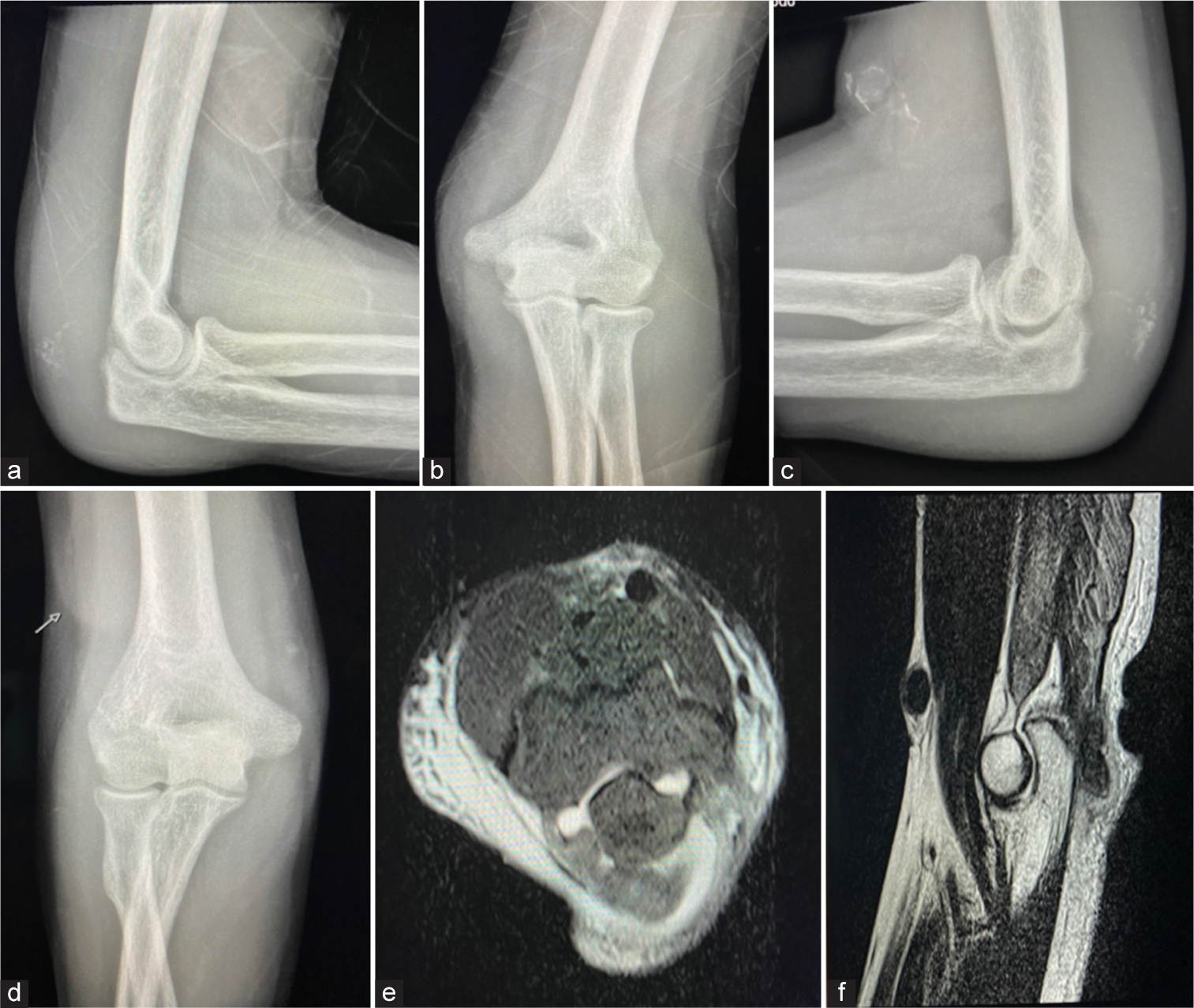
- (a and b) Left, (c and d) Right X-rays of elbows show effusion, fat pad sign with soft-tissue swelling and calcification over distal triceps (arrow), more obvious on the right side. (e and f) Are magnetic resonance imaging axial and sagittal cuts with a complete triceps tendon tear.
The diagnosis was made, and after patient counseling with treatment options with risks and benefits, the surgical option was decided. The patient did pre- and post-operative hemodialysis sessions and was optimized perioperatively. Under general anesthesia in the supine position, he underwent simultaneous repair of all ruptured tendons, starting with the left elbow and right knee, then the right elbow, by two surgical teams. Surgical fields were draped, and tourniquets were utilized. The knee was approached with a midline longitudinal incision, and the quadriceps tendon was identified. It was completely avulsed, with poor tendon quality, and poor bone quality of the patella plus patellar tendon was observed. After trimming the edges of the quadriceps tendon and refreshing the upper pole of the patella using a burr, Krackow’s suturing technique was utilized to place two fiber tapes size 2 mm medially and laterally through the quadriceps tendon. Three tunnels were drilled through the patella, and tapes were inserted through the tunnels. The patellar tendon was augmented with a fiber wire suture size of 2 mm and was inserted through the same tunnels. A 4-hole mini-plate was applied over the patella, and tape ends of the quadriceps tendon were inserted through and tensioned over the plate, and the same thing for the patellar tendon augment. The stability of the repair and patellar tracking were excellent. The retinaculum was repaired with heavy absorbable sutures.
Regarding the tricep tendons, each was approached through a posterior curvilinear incision centered over the olecranon. At the same time, the arm on the patient’s chest and the same steps were done bilaterally, except that the tourniquet was not utilized on the right side due to the presence of an arteriovenous (AV) fistula. Similarly, the quality of avulsed tendons and the bone was poor. The repair was done similarly to the knee utilizing two fiber tapes size 2 mm with Krackow’s technique, which was passed through intraosseous tunnels and tensioned over mini-fragment plates medially and laterally. Due to the weak and poor bone quality, anchors and transosseous tunnels alone were not strong enough. The plate was used to tie the tape and wire over so as not to weaken the bone further.
Adequate excursion with up to 100° of flexion was achieved without any significant tension on the repair. Limbs were splinted, with a long bivalved cast applied over the left upper limb at 30° of flexion, a long backslap over the right lower limb in the extended position, and the right upper limb due to AV fistula at 30°. The stability of repairs was also satisfactorily evident on post-operative radiographs [Figures 3 and 4].
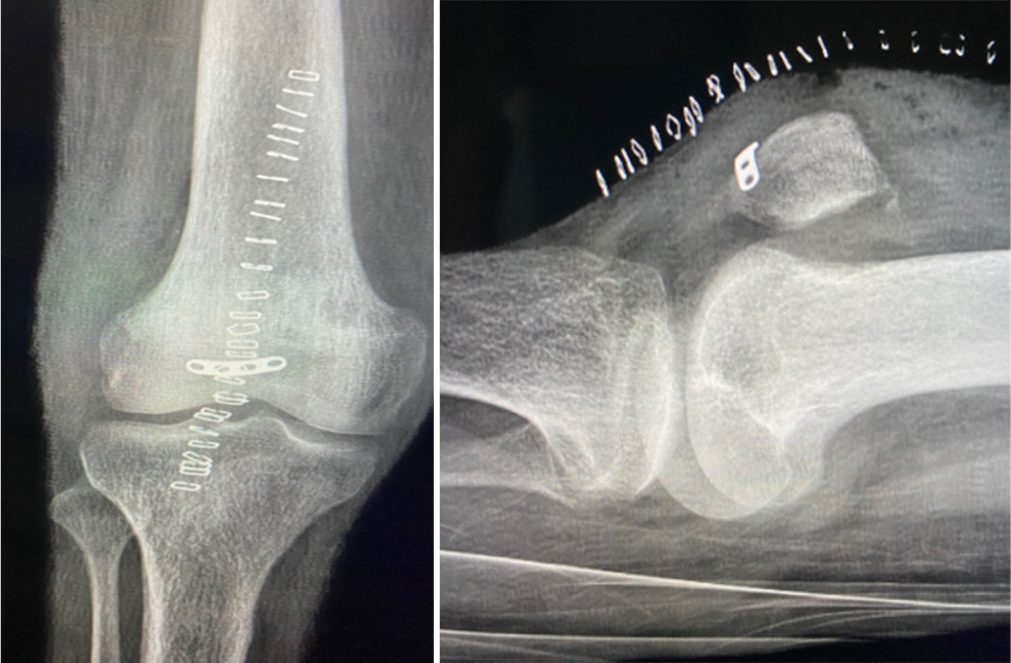
- Post-operative radiographs of the right knee.
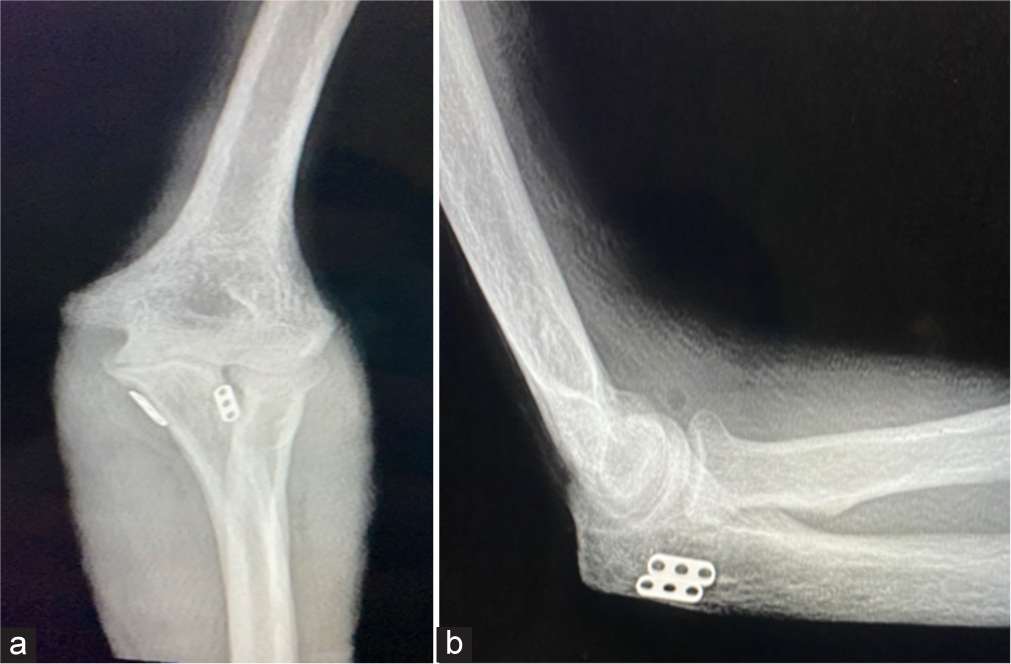
- (a and b) Post-operative radiographs of the elbows. b
Our rehabilitation protocol was non-weight-bearing with bed-to-chair transfer for the first two weeks post-operative for all the limbs. Knee rehabilitation continued non-weight-bearing for an additional 10 weeks in extension with gradual progressive flexion and extension started five weeks post-operative, then gradual weight-bearing started 10 weeks post-operative. Elbow rehabilitation consisted of a gradual ROM in a hinged brace starting two weeks postoperative (15° of flexion each week), totaling six weeks in a brace.
The patient was followed up in the clinic over four months, with the following detailed visits: (a) A two-week visit, wound check, and brace application of elbows, (b) A three-week visit, stitches/clips removal, and cylindrical cast application for the knee, (c) A six-week visit, cast removal, and brace application for the knee, (d) A 10-week visit, functional, active ROM was achieved (elbows: 0–130 bilaterally, knee: 10–90°) with all braces off, and (e) A 16-week visit, (right elbow: 5–130, left elbow 0–140, knee: full ROM with intact extensor mechanism) [Figure 5].

- Last visit (16 weeks) clinical photographs show (a-d) range of motion and (e) intact extensor mechanism.
DISCUSSION
Severely disabled patients with different chronic metabolic diseases, such as systemic lupus erythematosus, gout, rheumatoid arthritis, and chronic renal failure, can suffer from spontaneous tendon rupture, which is considered a rare complication.[1] Particularly in patients with chronic renal disease, the exact mechanism contributing to tendon rupture is unclear. However, researchers have believed that secondary hyperparathyroidism caused by hemodialysis plays a major role.[2] It has been reported that 15% of patients with chronic kidney disease on hemodialysis suffer from spontaneous tendon ruptures involving the triceps, quadriceps, and finger tendons due to uremic tendinopathy.[5]
Chronic hemodialysis leads to patients being uremic, which is usually due to abnormal calcium-phosphorus metabolism, which causes secondary hyperparathyroidism. This, in turn, leads to ligament and tendon tissue degradation due to high parathyroid hormone and a decrease in vitamin D levels.[3] Secondary hyperparathyroidism is the main reason for tendon ruptures in patients with chronic renal failure on hemodialysis. However, other factors are also attributed to tendon ruptures, including patients who are on corticosteroids and fluoroquinolones.[1]
Diagnosis is mostly clinical. Patients will present with a history of minimal trauma, pain, and inability to extend the joint. Upon examination for quadriceps rupture, a defect to the superior pole of the patella is palpated, and loss of the extensor mechanism is usually present. Similarly, triceps tendon rupture can be detected by palpating a gap defect, a positive modified Thompson’s squeeze test, and an inability to extend the elbow against resistance.[6] Patella baja and/or osseous avulsion of the upper pole of the patella[7] and olecranon can be seen on radiographic images. MRI can be utilized to confirm diagnosis and differentiate between partial and complete tears.
Regarding management, early surgical repair is the best intervention for quadriceps tendon rupture to recover its function due to less fibrosis and retraction.[3] Regarding triceps tendon rupture, improved outcomes have been reported in patients who underwent tendon repair.[1] Multiple surgical techniques have been utilized, such as transosseous, anchor sutures, and augmentation with tendon or ligament grafts for chronic tears. However, no specific treatment guideline was established.[8]
To our understanding, no recent study has been found in the literature addressing a case of bilateral triceps tendon rupture associated with unilateral quadriceps tendon rupture in a chronic renal disease patient. This article, along with previous reports, shows the ease of tendon ruptures with minor trauma and highlights the importance of taking preventive measures in such a susceptible group of patients.
CONCLUSION
Patients with chronic metabolic diseases, such as chronic renal failure, are at risk of developing spontaneous tendon ruptures. The exact mechanism contributing to tendon rupture in patients with chronic renal disease is unclear. Uremia and secondary hyperparathyroidism caused by hemodialysis play a significant role. Other contributing factors include corticosteroids and fluoroquinolones. Early surgical repair of ruptured tendons improved outcomes. Further larger studies are needed to confirm these observations.
Authors’ contributions
RKB, IAH, and AMM: Contributed to literature search, data acquisition, data analysis, manuscript preparation, and manuscript editing and review. TMR: Contributed to manuscript editing and review. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published, and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Conflicts of interest
There are no conflicting relationships or activities.
Financial support and sponsorship: This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Spontaneous tendon ruptures in patients with end-stage renal disease. Kidney Blood Press Res. 2009;32:32-6.
- [CrossRef] [PubMed] [Google Scholar]
- A simultaneous bilateral quadriceps and patellar tendons rupture in patients with chronic kidney disease undergoing long-term hemodialysis: A case report. BMC Musculoskelet Disord. 2020;21:179.
- [CrossRef] [PubMed] [Google Scholar]
- A simultaneous rupture of the patellar tendon and the contralateral quadriceps tendon in a patient with chronic renal failure undergoing long term hemodialysis. Med Arch. 2021;75:317-20.
- [CrossRef] [PubMed] [Google Scholar]
- The surgical management of distal triceps tendon ruptures: A systematic review. J Shoulder Elbow Surg. 2022;31:217-24.
- [CrossRef] [PubMed] [Google Scholar]
- Complete tricepspeesruptuur [Complete triceps tendon rupture; a rare tendon injury] Ned Tijdschr Geneeskd. 2018;162:D2744.
- [Google Scholar]
- Bilateral quadriceps tendon rupture as the presenting manifestation of chronic kidney disease. Indian J Nephrol. 2011;21:48-51.
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral, spontaneous and simultaneous rupture of the quadriceps tendon in chronic renal failure and secondary hyperparathyroidism. Report of five cases. Arch Anat Cytol Pathol. 1991;39:228-32.
- [Google Scholar]
- Triceps tendon rupture: Repair and rehabilitation. Shoulder Elbow. 2018;10:62-5.
- [CrossRef] [PubMed] [Google Scholar]




