
Translate this page into:
Effects of abdominal bracing maneuver during walking on trunk muscle endurance in healthy staff of Northwest Institute: A randomized controlled pilot study
 DPT, MS OMPT., Syed Zain Ul Abidin1DPT, MS MSK.
DPT, MS OMPT., Syed Zain Ul Abidin1DPT, MS MSK.
*Corresponding author: Uzair Ahmad, Assistant Professor, Department of Physical Therapy, Northwest Institute of Health Sciences, Peshawar, Pakistan. azmatuzair125@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mumtaz H, Durani A, Shoaib W, Ahmad U. Abidin S. Effects of abdominal bracing maneuver during walking on trunk muscle endurance in healthy staff of Northwest Institute: A randomized controlled pilot study. J Musculoskelet Surg Res. 2024;8:264-71. doi: 10.25259/JMSR_82_2024
Abstract
Objectives:
This study aimed to find the effect of abdominal bracing (AB) maneuver during walking on trunk muscle endurance in healthy individuals.
Methods:
A randomized control pilot study was conducted at Northwest Institute of Health Sciences Peshawar from July to December 2023. A total of 32 participants aged 25–40 were randomized to Groups A and B. Group A received AB maneuver with walking, while Group B received walking only. Both groups received a total of 12 sessions. Pre- and post-endurance testing was performed using McGill’s Torso Muscular Endurance Test.
Results:
The mean age of participants in Group A was 29.06 ± 5.14 years, while the mean age of participants in Group B was 27.62 ± 2.84 years. The mean and standard deviation of the flexor endurance test between Groups A and B after treatment were 27.37 ± 3.26 and 16.21 ± 2.24, respectively. A significant difference was observed in flexor endurance and right and left lateral flexor endurance between the two groups (P < 0.05). In contrast, no significant difference was observed in extensor endurance between the two groups, having P > 0.05. Within-group analysis in Group A revealed a significant difference in pre-post-intervention flexion, right and left lateral flexors, and extensors (P < 0.05). However, within-group analysis in Group B revealed a statistical difference in flexors endurance, which is not clinically significant.
Conclusion:
The AB maneuver with walking compared with walking alone may improve the endurance of the trunk flexors, specifically the right and left lateral flexors.
Keywords
Abdominal bracing
Core muscles
Physical activity
Trunk muscle endurance
Walking exercise

INTRODUCTION
The term core is a muscular unit resembling a box, where the front is formed by abdominal muscles, the back consists of paraspinal and gluteal muscles, the roof is represented by the diaphragm, and the bottom includes the pelvic floor and hip girdle muscles. Enclosed within this structure is a total of 29 pairs of muscles, which play a key role in stabilizing the spine pelvis and the kinetic chain during various functional movements.[1] These muscles are crucial for enabling fundamental body movements, offering both stability and strength during different activities. One significant function of these muscles is to keep the body straight.[2] The endurance of core muscles has been correlated with changes in spinal stability.[3] When the core muscles are weakened, it results in spinal instability. It is associated with an elevated burden on the spine, as well as an increased likelihood of experiencing low back pain (LBP).[4] The core muscle endurance or trunk muscle endurance refers to the capacity of muscles to maintain their activity over an extended duration. Core muscle endurance is linked to various conditions, such as LBP, postural abnormalities, and impaired balance across different populations.[5] Spinal musculoskeletal conditions are highly prevalent, constituting approximately 21% of all global disability cases. Among these conditions, LBP and neck pain continue to be the foremost contributors to the burden on musculoskeletal health and remain the leading cause of disability worldwide.[6] Approximately 80% of adults are estimated to have at least one instance of LBP during their lifetime.[7] Trunk training can be used both as a preventive measure and as a treatment approach for addressing LBP.[4] Abdominal hollowing (AH) and abdominal bracing (AB) maneuvers are commonly advised techniques for stabilizing the trunk muscles and minimizing undesired pelvic movement during movement activities.[8]
Abdominal co-contraction, also known as bracing, is widely recognized as one of the most efficient approaches to enhance trunk stability. It is frequently recommended and incorporated into rehabilitation and fitness programs.[9] Walking is a strongly recommended rehabilitative activity for individuals with LBP due to its cost-effectiveness and potential to improve isometric endurance by increasing muscular endurance.[10] It is widely favored as a physical activity due to its universal accessibility, minimal skill requirements, and low likelihood of causing injuries.[11] The previous studies have investigated AB and AH maneuvers on individuals across a range of body positions, including standing to supine position,[12] quadruped position,[13] side lying,[14] and standing in place.[15] They found that AB may enhance the muscle activity of the transverse abdominis, quadratus lumborum, external oblique, and internal oblique muscles. Similarly, a cross-sectional study (2022) found that walking with AB can increase the activity of trunk muscles.[16] However, there is a lack of experimental studies conducted on individuals with AB during flat walking. Therefore, our study aimed to determine the effects of AB maneuver during walking on trunk muscle endurance in healthy staff at Northwest Institute, Peshawar.
MATERIALS AND METHODS
Participants
A randomized controlled pilot study was conducted on healthy individuals at Northwest Institute of Health Sciences from July to December 2023. The OpenEpi tool was used to calculate sample size with a 95% confidence interval and 80% of study power. The parameters used for sample size were the mean and standard deviation (SD) of pre-rectus abdominis muscle activity (404.96 ± 65.79 Millivolt) for Group A, mean and SD of post-rectus abdominis muscle activity (478.22 ± 79.31 Millivolt) for Group B were taken from a previous study.[17] The calculated sample size was (n = 32), and 16 participants were randomly allocated to each group using the lottery method. The participants were selected through non-probability purposive sampling. The inclusion criteria were both male and female employees of Northwest Institute of Health Sciences with ages ranging from 25 to 40 years, having no congenital defects, orthopedic disorders, or deformities in upper or lower extremities, and being able to walk normally. Individuals with moderate or low levels of physical activity based on the International Physical Activity Questionnaire-Short Form (IPAQ-SF) and individuals who are safe to perform exercises based on the Physical Activity Readiness Questionnaire (PAR-Q) were included in this study. The exclusion criteria were individuals who had prior surgery of the lower extremities and/or spine, any musculoskeletal conditions affecting the spine and/or extremities, or individuals with any medical conditions such as hypertension or cardiovascular disease that can affect the performance of the exercise protocol.
Procedure
A total of 32 individuals were randomly allocated in each group, 16 in Group A and 16 in Group B, as shown in Figure 1. Both groups received the intervention thrice a week for 4 weeks (12 sessions).[18] Group A had to do the AB maneuver while walking on a flat surface, while Group B received walking on a flat surface only. Walking protocol for both groups following the frequency, intensity, type, and time principle included a warm-up for 5 min with a 10-min walk (week 1), 15 min walk (week 2), and a walk for 20 min (weeks 3–4),[19] as shown in Table 1.
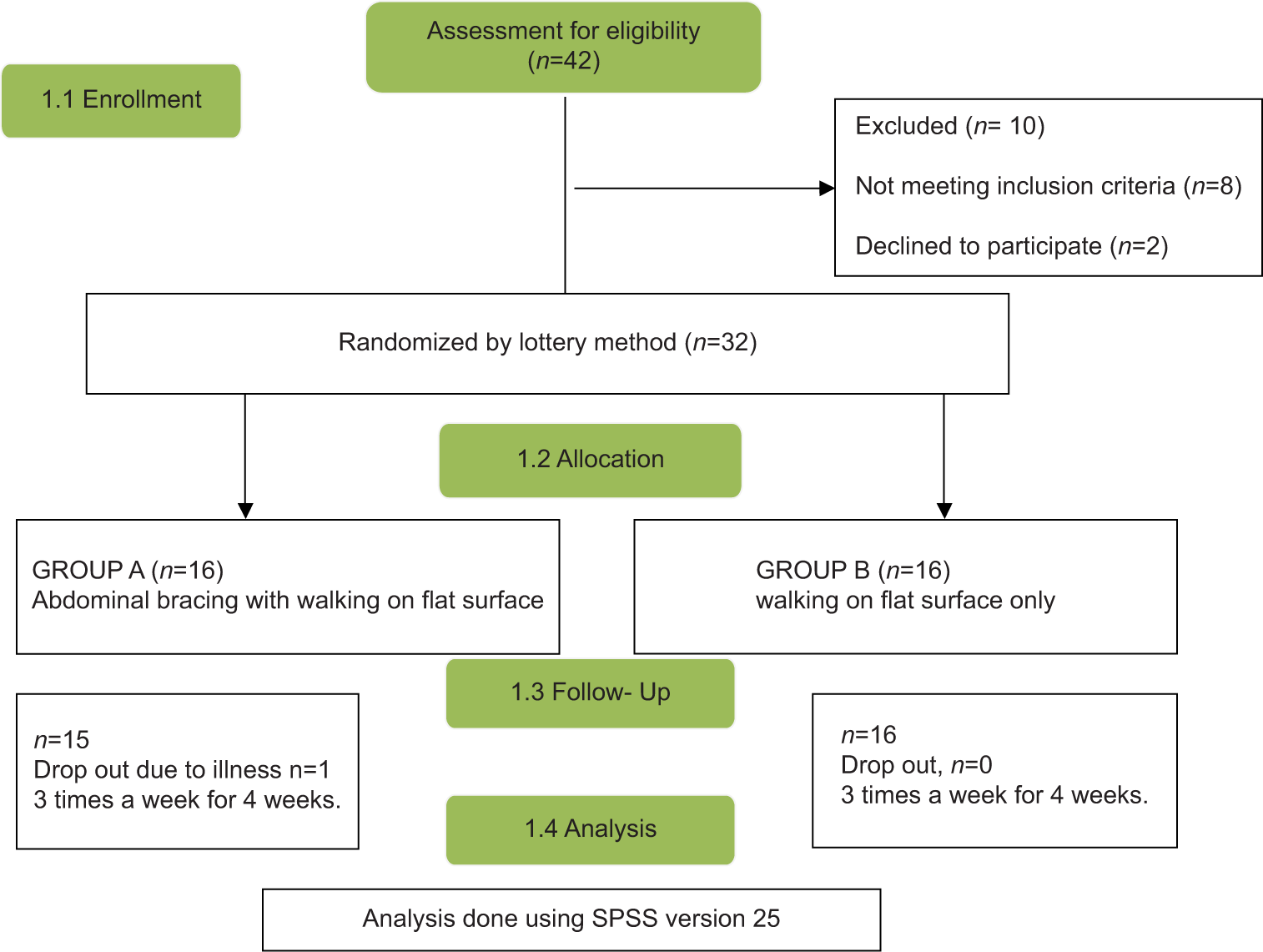
- CONCORT flow diagram.
| Frequency | 3 times a week for 4 weeks |
|---|---|
| Intensity | Moderate intensity walking, 50–60% of maximum heart rate |
| Time | 5 min warm up |
| 10 min (week 1) | |
| 15 min (week 2) | |
| 20 min (week 3-4) | |
| Type | Walking with abdominal bracing maneuver |
FITT: Frequency, intensity, time, type
Outcome measures
The pre- and post-measurements were taken using the following tools. IPAQ-SF was used to screen the participants for physical activity. It is concise and widely utilized to assess self-reported physical activity among the general adult population.[20] The self-administered IPAQ-SF has acceptable reliability and validity.[21] Based on IPAQ-SF, individuals with moderate to low physical activity levels were included in the study. We did not include individuals with high levels of physical activity. This decision was made to ensure consistency in the study population and minimize confounding variables. High levels of physical activity may indicate a different baseline fitness and muscle endurance level, potentially affecting the study outcomes.
The PAR-Q, consisting of seven items, serves as a questionnaire for screening individuals who may be at risk of experiencing adverse effects due to increased physical activity, particularly those with heart problems.[22]
A Pressure Biofeedback Unit was used to instruct the participants on effective AB maneuvers.[19] Participants were instructed to recline on a stable surface with their knees bent at 90° and their unit positioned beneath the 5th lumbar vertebrae. They were asked to contract the abdominal muscle until the pressure reached 40 mm hg and maintain this pressure. The participants drew their navel inward and backward toward the lumbar region, creating a slightly concave abdomen while breathing normally.[17]
McGill’s torso muscular endurance test measured trunk muscle endurance. It consists of four isometric tests: flexion, extension, left lateral flexion, and right lateral flexion. McGill’s tests are the most reliable core endurance tests and are popular in clinical settings for assessing the isometric endurance of core muscles, as shown in Figure 2.[23]
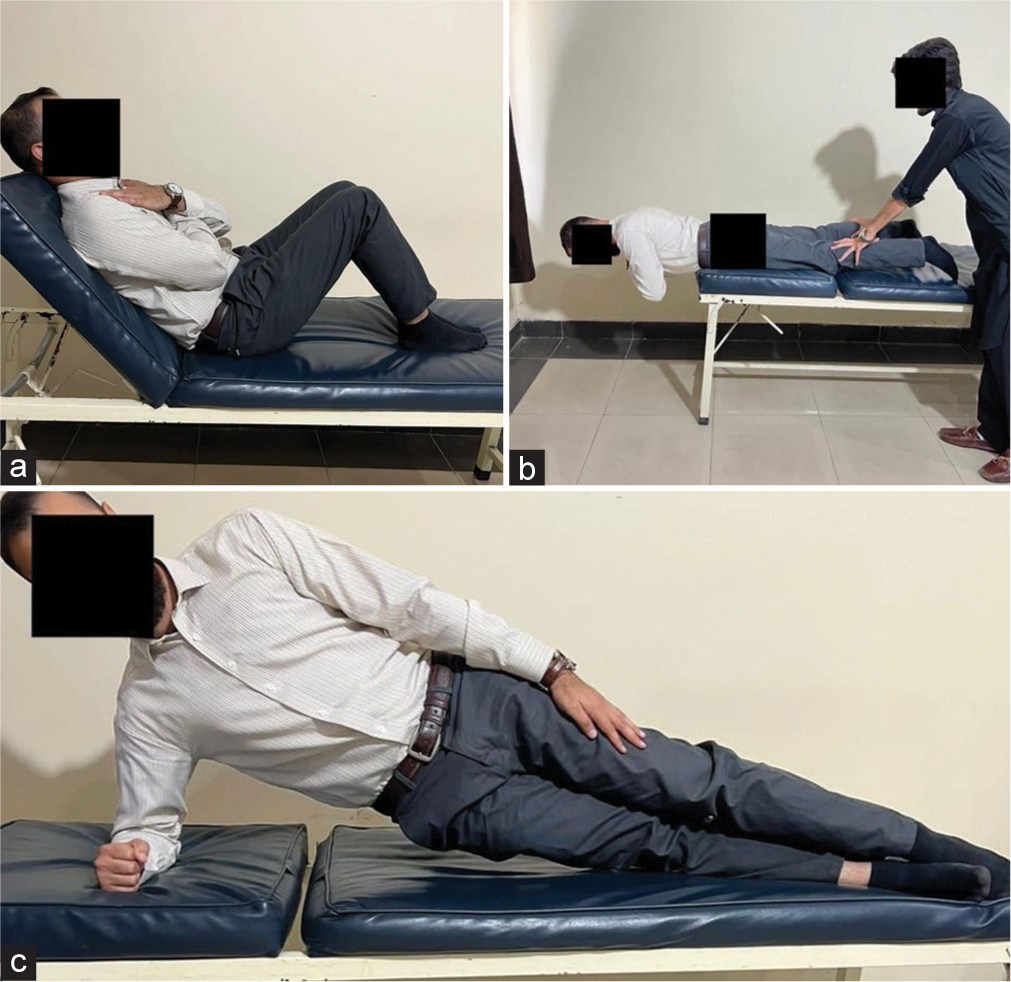
- McGill’s torso muscular endurance test. (a) The trunk flexor endurance test, (b) the extensor endurance test, and (c) the lateral flexor endurance test.
For the trunk flexor endurance test, participants were instructed to sustain a neutral spine position following the removal of the board until they felt fatigued in their activated abdominal muscles or noticed their back arching. The test concluded on detecting an obvious trunk or spinal position alteration. The goal was to sustain this posture without back support for as long as possible. A stopwatch was used to record the duration from the moment the board was removed until the test ended [Figure 2a].[19] For the trunk lateral flexor endurance test, when prepared, the participant adopted a full side bridge stance, extending both legs and placing the sides of feet on the ground. The lower arm’s elbow was directly beneath the shoulder, forearm facing outward, while the upper arm rested beside the body. The objective was to lift the hips off the mat, achieving a straight body alignment supported solely by the feet and forearm. The aim was to maintain this position for an extended duration. A stopwatch was initiated on assuming the side bridge posture and stopped when the position was no longer sustained. The duration was recorded, and the test was repeated on opposite sides using the same procedure [Figure 2b].[19] For the trunk extensor endurance test, the objective for the participant was to sustain a horizontal, prone posture for the longest duration possible. Upon readiness, the subject lifted their torso until it was parallel to the floor, aligning with their legs. They then crossed their arms over their chests. The stopwatch began when this position was assumed. The test concluded when the participant could no longer sustain the posture, at which point the time was recorded [Figure 2c].[19]
Statistical analysis
The data analysis used Statistical Package for the Social Sciences version 25. The normality test was conducted using the Shapiro–Wilk test. The data exhibited a normal distribution, so parametric tests were applied. The comparison between groups was done using an independent t-test, and within groups, a comparison was done using a paired t-test.
RESULTS
Out of the 32 participants, 16 participants (50%) were assigned to Group A, while the other 16 participants (50%) were designated to Group B. There was one dropout from Group A. Out of the total, 8 were female and 23 were male. Group A had 12 males and three females with a mean age of 29.06 ± 5.14 years. Group A’s body mass index (BMI) score was 24.85 ± 5.34 kg/m2, while Group B had 11 males and five females with a mean age of 27.62 ± 2.84 years. Group B’s BMI score was 24.04 ± 4.75 kg/m2 [Table 2].
| Variables | Mean±Std | |
|---|---|---|
| Group A (n=15) |
Group B (n=16) |
|
| Age (years) | 29.06±5.14 | 27.62±2.84 |
| Height (meter) | 1.69±0.07 | 1.70±0.09 |
| Weight (kilogram) | 71.46±14.60 | 69.93±16.69 |
| BMI (kg/m2) | 24.85±5.34 | 24.04±4.75 |
| PAR-Q questions 1–7 | ||
| Yes (Frequency (%) | 0 | 0 |
| No (Frequency (%) | 15 (100) | 16 (100) |
| 1Level of Physical Activity (Frequency (%) | ||
| Low (Not meeting the criteria of Moderate and High) | 10 (66.6) | 12 (75) |
| Moderate (≥600 MET- minutes/week) | 5 (33.3) | 4 (25) |
| High (≥3000 MET-minutes/week) | 0 | 0 |
Std: Standard deviation, BMI: Body mass index, PAR-Q: Physical activity readiness questionnaire, International physical activity questionnaire1, MET: Metabolic equivalent
Between-groups analysis
Since the test indicated a normal distribution of data, we proceeded to compare groups using a parametric test, specifically the independent t-test.
Before treatment, no significant difference was observed in flexors, left and right lateral flexors and extensor endurance between the two groups, with P > 0.05. After treatment, a significant difference was observed in flexor endurance, right lateral flexor endurance, and left lateral flexor endurance between the two groups, with (P < 0.05). However, no significant difference was noticed in extensor endurance between the two groups, with (P > 0.05), [Table 3 and Figure 3].
| Variables | Group | N | Mean±Std | Mean diff | aP-value |
|---|---|---|---|---|---|
| Pre-intervention flexor endurance test | Group A | 15 | 15.94±2.68 | 0.84 | 0.342212 |
| Group B | 16 | 15.10±2.16 | |||
| Post-intervention flexor endurance test | Group A | 15 | 27.37±3.26 | 11.15 | 0.000 |
| Group B | 16 | 16.21±2.24 | |||
| Pre- intervention right lateral flexor endurance test | Group A | 15 | 10.95±2.40 | 0.07 | 0.928015 |
| Group B | 16 | 10.88±2.23 | |||
| Post- intervention right lateral flexor endurance test | Group A | 15 | 23.64±3.14 | 11.28 | 0.000 |
| Group B | 16 | 12.36±2.16 | |||
| Pre- intervention left lateral flexor endurance test | Group A | 15 | 10.79±3.19 | -0.34196 | 0.757221 |
| Group B | 16 | 11.14±2.90 | |||
| Post- intervention left lateral flexor endurance test | Group A | 15 | 23.43±3.05 | 10.80 | 0.000 |
| Group B | 16 | 12.63±2.53 | |||
| Pre- intervention extensor endurance test | Group A | 15 | 16.60±3.56 | -0.66 | 0.556400 |
| Group B | 16 | 17.26±2.62 | |||
| Post- intervention extensor endurance test | Group A | 15 | 19.94±3.27 | 2.08 | 0.078795 |
| Group B | 16 | 17.85±3.10 |
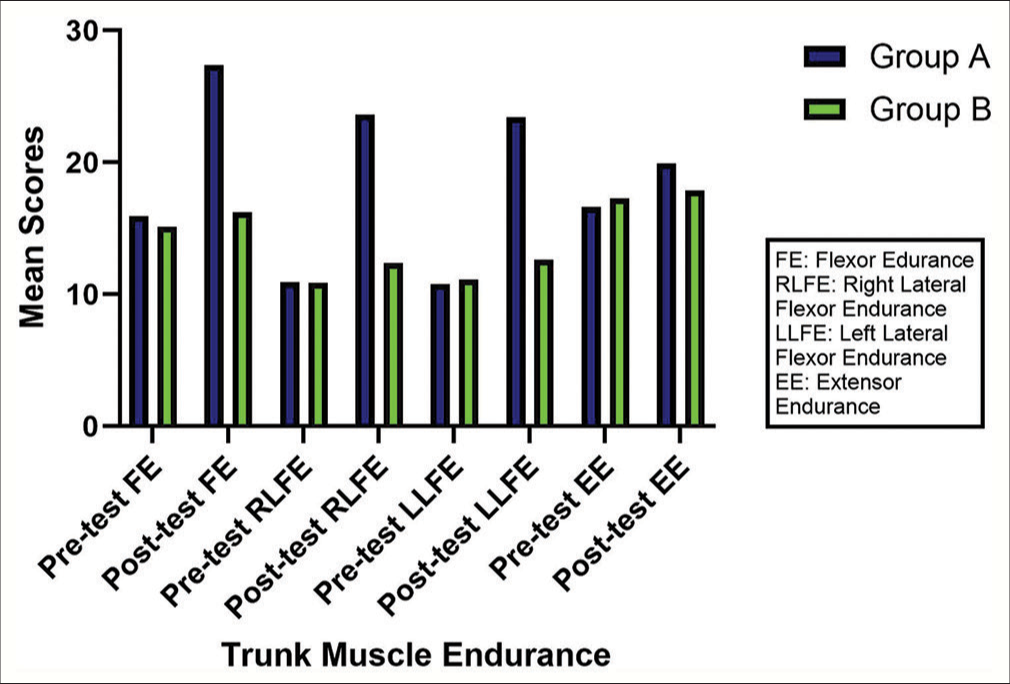
- Trunk muscle endurance between group A and B.
Within-group analysis
Since the test indicated a normal data distribution, we utilized a parametric test, specifically the paired t-test, for comparison within groups.
Group A
Within-group analysis revealed a significant difference in Group A’s pre- and post-intervention flexor endurance, with (P < 0.05). In addition, after treatment, a significant difference was observed in Group A’s pre- and post-intervention right lateral flexor endurance (P < 0.05). Similarly, a significant difference was observed in Group A’s pre- and post-intervention left lateral flexor endurance, with P < 0.05. Moreover, a significant difference was observed in pre- and post-intervention extensor endurance of Group A, with P < 0.05 [Table 4].
| Variables | n | Mean±Std | Mean diff | aP-value |
|---|---|---|---|---|
| Pair 1 | ||||
| Pre- intervention flex endurance test | 15 | 15.94±2.68 | −11.42 | 0.000 |
| Post- intervention flex endurance test | 15 | 27.37±3.26 | ||
| Pair 2 | ||||
| Pre- intervention right lateral flexor endurance test | 15 | 10.95±2.40 | −12.69 | 0.000 |
| Post- intervention right lateral flexor endurance test | 15 | 23.64±3.14 | ||
| Pair 3 | ||||
| Pre- intervention left lateral flexor endurance test | 15 | 10.79±3.19 | −12.63 | 0.000 |
| Post- intervention left lateral flexor endurance test | 15 | 23.43±3.05 | ||
| Pair 4 | ||||
| Pre- intervention extensor endurance test | 15 | 16.60±3.56 | −3.34 | 0.000157 |
| Post- intervention extensor endurance test | 15 | 19.94±3.27 |
Group B
After treatment, a significant difference was observed in Group B’s pre- and post-intervention flexor endurance, with P < 0.05. However, although statistically significant, it may not be considered clinically significant as the mean difference was −1.11. In addition, after treatment, a significant difference was observed in the pre- and post-intervention right lateral flexor endurance and left lateral flexor endurance of Group B, with P < 0.05. However, as with lateral flexor endurance, these differences may not be considered clinically significant due to mean differences of −1.48 and −1.49, respectively. Furthermore, after treatment, no significant difference was observed in the pre- and post-intervention extensor endurance of Group B, with P > 0.05 [Table 5].
| Variables | n | Mean±std | Mean diff | aP-value |
|---|---|---|---|---|
| Pair 1 | ||||
| Pre- intervention flexor endurance test | 16 | 15.10±2.16 | −1.11 | 0.000 |
| Post- intervention flexor endurance test | 16 | 16.21±2.24 | ||
| Pair 2 | ||||
| Pre- intervention right lateral flexor endurance test | 16 | 10.88±2.23 | −1.48 | 0.000 |
| Post- intervention right lateral flexor endurance test | 16 | 12.36±2.16 | ||
| Pair 3 | ||||
| Pre- intervention left lateral flexor endurance test | 16 | 11.14±2.90 | −1.49 | 0.000 |
| Post- intervention left lateral flexor endurance test | 16 | 12.63±2.53 | ||
| Pair 4 | ||||
| Pre- intervention extensor endurance test | 16 | 17.26±2.62 | −0.58 | 0.362123 |
| Post- intervention extensor endurance test | 16 | 17.85±3.10 |
DISCUSSION
Our study aimed to find the effect of AB maneuvers during walking on trunk muscle endurance in healthy individuals. Group A, which received the AB maneuvers with walking, showed a significant difference in pre- and post-intervention endurance of trunk muscles. Meanwhile, the walking alone group (Group B) showed no clinical significance in pre- and post-intervention endurance of trunk flexors and right and left lateral flexors. No significant difference was observed in Group B’s pre- and post-intervention extensor endurance. These results were supported by a randomized control trial conducted by Olowe et al. (2021), which indicated more favorable outcomes regarding the enhanced endurance of trunk muscles in individuals who underwent treadmill walk exercise with core muscle activation compared to those who underwent treadmill walk without core muscle activation and the control group.[19]
Our study demonstrated that the AB maneuvers, when combined with walking, led to enhanced endurance in trunk flexors, trunk lateral flexors, and trunk extensors, including transverse abdominis, internal and external obliques, and multifidus in healthy individuals. These findings are supported by Ahn et al. (2020), who investigated the effects of AB during flat walking on trunk muscle activity of trunk and legs. This study was also performed in healthy individuals with no LBP and it was concluded that engaging in level walking while actively employing the AB technique led to a significant increase in muscle activity of the rectus abdominis, external obliques, latissimus dorsi, and vastus medialis.[24]
Another study conducted by Olowe et al. in 2022 showed that lumbar stabilization exercises have been shown to be superior to treadmill walking exercises in terms of effectiveness in activating the multifidus muscle, reducing pain intensity, and decreasing functional disability in people dealing with chronic mechanical LBP. However, direct measurement of the multifidus muscle’s electromyography (EMG) activity through needle insertion was not included due to the painful nature of the procedure. The study could not measure the EMG activity of the multifidus muscle during dynamic movement.[18] Similarly, our study concluded that the individuals who had received AB along with walk showed significance in endurance of multifidus along with other trunk extensors, including erector spinae, longissimus, and iliocostalis in contrast to the group who had walked only.
It is also advisable to sustain the AB maneuver contraction during ramp walking as a training method to enhance musculoskeletal function.[25] Similarly, the importance of AB maneuvers with ascending stairs was highlighted in a study that showed that ascending stairs while maintaining AB activation engages the abdominal muscles, enhancing trunk balance and lumbar stability. This dual action reduces excessive lumbar lordosis and pelvic anterior tilt, ultimately improving the musculoskeletal system’s function,[17] while our study showed the importance of combining AB maneuver during gait on trunk muscles endurance.
Stabilization exercises play a key role in enhancing endurance and overall physical performance. The stabilization exercise used in our study was the AB maneuver, which showed the significance of the stabilization exercise when combined with gait. Our study reported that the pre- and post-intervention evaluation of the group that received AB maneuver with walking had improved trunk endurance. This study was conducted in a healthy population. Studies have indicated core stabilization exercises’ significance and effectiveness in LBP patients. Core stability exercises were proven efficient in enhancing functionality, relieving pain, and improving endurance among patients with lumbar disc herniation and LBP.[26,27] The core stabilization, when combined with the ADIM technique, was demonstrated to offer a protective effect against the harmful decrease in stature change and trunk muscle fatigue during an extended period of sitting.[28]
A study conducted by Kim and Park (2020) concluded that utilizing the AB technique along with elevating the angle between the ground and the humerus might prove to be a beneficial exercise method for boosting the activity of abdominal muscles.[29]
The importance of AB maneuver has also been highlighted by various studies during plank positions. Incorporating the AB maneuver into the prone plank exercise proves to be an effective method for enhancing abdominal activity, especially in the internal and external oblique muscles. This approach achieves optimal activity levels within both the local and global stabilizing systems. However, this study was limited to healthy people without any LBP and disorders.[30] Similarly, our study demonstrated that the healthy population showed enhanced endurance of trunk muscles, including transverse abdominis, multifidi, and the internal and external obliques, when combined with walking.
Limitations
This study has certain limitations. Future studies can focus on AB during treadmill walks and patients with LBP. The sample size can be increased for better external validity. Furthermore, different abdominal waist sensors can also be used in future studies to see waist circumference changes and effective AB.
CONCLUSION
This study concluded that participants who received AB with walking showed more improvement in the endurance of trunk flexors, right and left flexors, and trunk extensor muscles than participants who had walked alone.
AUTHORS’ CONTRIBUTIONS
HM, AD, and WS contributed to the study’s design, literature search, clinical studies, and data acquisition. UA contributed to conceptualization, statistical analysis, manuscript preparation, and manuscript editing. SZA contributed to the revision and final approval of the manuscript. All authors critically reviewed and approved the final draft and are responsible for the manuscript’s content and its similarity index.
ETHICAL APPROVAL
The research was conducted per the principles outlined in the Declaration of Helsinki and received approval from the Institutional Research Board and ethical committee of Northwest Institute and Northwest General Hospital and Research Center Peshawar, Pakistan. (IRB&EC/2023-HIS/055).
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate participants consent forms. In the form, the participants have given their consent for their images and other clinical information to be reported in the journal. The participants understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
ARTIFICIAL INTELLIGENCE (AI)-ASSISTED TECHNOLOGY FOR MANUSCRIPT PREPARATION
The authors affirm that artificial intelligence (AI)-assisted technology was not utilized in the writing or editing of the manuscript, and no images were manipulated using AI.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Core stability exercise principles. Curr Sports Med Rep. 2008;7:39-44.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of selected core strengthening workouts & Balanced diet in reducing weight among college teachers under Calicut University. Int J Physiol Nutr Phys Educ. 2020;5:109-12.
- [Google Scholar]
- Designing health-referenced standards for the plank test of core muscular endurance. Meas Phys Educ Exerc Sci. 2022;26:344-51.
- [CrossRef] [Google Scholar]
- Trunk muscle activity during trunk stabilizing exercise with isometric hip rotation using electromyography and ultrasound. J Electromyogr Kinesiol. 2019;49:102357.
- [CrossRef] [PubMed] [Google Scholar]
- Association of core muscle endurance times with balance, fatigue, physical activity level, and kyphosis angle in patients with ankylosing spondylitis. J Clin Rheumatol. 2022;28:e135-40.
- [CrossRef] [PubMed] [Google Scholar]
- Practicable performance-based outcome measures of trunk muscle strength and their measurement properties: A systematic review and narrative synthesis. PLos One. 2022;17:e0270101.
- [CrossRef] [PubMed] [Google Scholar]
- Abdominal trunk muscle weakness and its association with chronic low back pain and risk of falling in older women. BMC Musculoskelet Disord. 2019;20:273.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of abdominal hollowing and bracing maneuvers on trunk muscle activity and pelvic rotation angle during leg pull front pilates exercise. Healthcare (Basel). 2022;11:60.
- [CrossRef] [PubMed] [Google Scholar]
- Trunk muscle activities during abdominal bracing: Comparison among muscles and exercises. J Sports Sci Med. 2013;12:467-74.
- [Google Scholar]
- The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine (Baltimore). 2019;98:e16173.
- [CrossRef] [PubMed] [Google Scholar]
- Walking for fitness: A case study on the experiences, challenges, and perceived benefits from regular walking exercise of young adult. Int J Soc Sci Educ Res Stud. 2021;1:42-9.
- [Google Scholar]
- Effects of abdominal hollowing and bracing maneuvers on hip extension strength in prone standing position. Isokinetics Exerc Sci. 2020;28:161-9.
- [CrossRef] [Google Scholar]
- Comparison of the recruitment of transverse abdominis through drawing-in and bracing in different core stability training positions. J Exerc Rehabil. 2019;15:819-25.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of abdominal hollowing and abdominal bracing during side-lying hip abduction on the lateral rotation and muscle activity of the pelvis. J Exerc Rehabil. 2018;14:226-30.
- [CrossRef] [PubMed] [Google Scholar]
- Abdominal bracing during lifting alters trunk muscle activity and body kinematics. Appl Ergon. 2017;63:91-8.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of the abdominal bracing maneuver on muscle activity of the trunk and legs during walking in healthy adults. Phys Ther Rehabil Sci. 2022;11:119-26.
- [CrossRef] [Google Scholar]
- The effects of abdominal drawing-in maneuver during stair climbing on muscle activities of the trunk and legs. J Exerc Rehabil. 2019;15:224-8.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of treadmill walk with abdominal bracing versus usual care on functional limitation and fear-avoidance behaviours in the management of non-specific low back pain-a randomized control study. Bull Fac Phys Ther. 2022;27:35.
- [CrossRef] [Google Scholar]
- Effects of combining core muscle activation with treadmill walk on endurance of trunk muscles: A pilot study. Niger J Exp Clin Biosci. 2021;9:37-46.
- [CrossRef] [Google Scholar]
- Criterion validity and reliability of the International Physical Activity Questionnaire-Hungarian short form against the RM42 accelerometer. BMC Public Health. 2021;21:381.
- [CrossRef] [PubMed] [Google Scholar]
- Validity and reliability of the International Physical Activity Questionnaire in college students. Am J Health Educ. 2006;37:337-43.
- [CrossRef] [Google Scholar]
- Which behaviour change techniques are effective to promote physical activity and reduce sedentary behaviour in adults: A factorial randomized trial of an e-and m-health intervention. Int J Behav Nutr Phys Act. 2020;17:27.
- [CrossRef] [PubMed] [Google Scholar]
- The number of repetitions of the McGill tests to reliably determine core muscle endurance in subjects with and without chronic nonspecific low back pain: A cross sectional study. Med Sci. 2019;23:452-61.
- [Google Scholar]
- Effects of abdominal drawing-in maneuver on muscle activity of the trunk and legs during flat walking. Korean Soc Phys Med. 2020;15:49-56.
- [CrossRef] [Google Scholar]
- The effects of abdominal drawing-in on muscle activity in the trunk and legs during ramp walking. PNF Mov. 2019;17:137-44.
- [Google Scholar]
- Effectiveness of spinal stabilization exercises with and without stretching of Latissimus dorsi Muscle in chronic mechanical low back pain. Rawal Med J. 2020;45:857-62.
- [Google Scholar]
- Effects of core stabilization exercises on low back pain, disability and back muscle endurance in patients with lumbar disc herniation. Ann King Edward Med Univ. 2023;29:123-8.
- [CrossRef] [Google Scholar]
- The effect of core stabilization exercise with the abdominal drawing-in maneuver technique on stature change during prolonged sitting in sedentary workers with chronic low back pain. Int J Environ Res Public Health. 2022;19:1904.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of the abdominal hollowing technique applied during plank exercises at different angles between ground and the humerus on abdominal stabilization muscle activity. J Korean Phys Ther. 2020;32:94-100.
- [CrossRef] [Google Scholar]
- Influence of abdominal hollowing maneuver on the core musculature activation during the prone plank exercise. Int J Environ Res Public Health. 2020;17:7410.
- [CrossRef] [PubMed] [Google Scholar]




