
Translate this page into:
Effects of board games on balance in association with cognition in community-dwelling older adults

*Corresponding author: Muhammad Ammar, Department of Physical Therapy, Post Grad Trainee at Pakistan Railway Hospital, Rawalpindi, Pakistan. ammarmuhammad5678@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ammar M, Amjad I, Nisar M, Ghoneim OS. Effects of board games on balance in association with cognition in community-dwelling older adults. J Musculoskelet Surg Res. 2024;8:256-63. doi: 10.25259/JMSR_122_2024
Abstract
Objectives:
Falls among the elderly are a prevalent concern. Maintaining balance and preventing falls necessitate cognitive processes, such as information processing speed and executive functions. The objective was to determine the impacts of board games on cognition, balance, and risk of falls among community-dwelling elders.
Methods:
Sixty-four elders aged 65 years and above, with mini–mental state examination (MMSE), scores above 26 and Berg balance scale (BBS) scores between 41 and 52, were recruited with a sample size of 64 divided into two groups, 32 in each group. Participants were randomized through the sealed envelope technique into experimental (engaging in board games) and control groups (not involved in board game activity). The BBS, MMSE, timed upand-go test (TUGT), and dynamic gait index (DGI) were assessed at baseline, four weeks, and eight weeks.
Results:
Participants engaging in board games (mean age 69.93 ± 4.77) demonstrated significant improvements in cognition, with MMSE scores increasing from 26.8 ± 0.83 at baseline to 28.6 ± 0.74 after eight weeks (P < 0.001). BBS scores enhanced from 47.2 ± 1.84 to 49.8 ± 5.15 (P < 0.001), DGI scores improved from 19.65 ± 1.49 to 21.37 ± 1.47 (P < 0.001), and TUGT scores decreased from 10.40 ± 0.69 to 10.22 ± 0.67 (P < 0.001). Mixed analysis of variance revealed significant differences between experimental and control groups for MMSE (P < 0.001), BBS (P < 0.001), DGI (P < 0.001), and TUGT (P < 0.001).
Conclusion:
The eight-week interactive physical-cognitive training program involving board games was found to enhance cognitive performance, mobility, and balance and decrease fall risk among the elderly.
Keywords
Board games
Balance
Cognition
Fall risk
Mobility

INTRODUCTION
Community-dwelling elderly are defined by their age (≥65 years of age) and by living independently. The engagement of geriatric adults in civic activities and local governance contributes to the democratic process. It ensures that community policies consider the needs of all age groups because they are active consumers and voters.[1] The geriatric population has to face various challenges, both physically and psychosocially. Some of the main issues are (a) health challenges (cognitive decline and chronic illnesses), (b) social isolation, (c) mental health issues, (d) limited access to health care, (e) nutritional challenges, and (f) falls. To address these challenges, a comprehensive and supportive approach is required among health-care professionals, community organizations, and policymakers to ensure good health and quality of life for senior citizens. Elderly falls pose a serious health risk. They can result in several issues, such as physical injuries (fractures and head injuries), functional decline, fear of falling, psychological problems, independence loss, social isolation, a decline in quality of life, hospitalization, and rehabilitation and a higher medical expenses. There are multi-factorial causes of falls, including physiological and cognitive elements. Although age is a factor in cognitive decline, falls were more common in older persons who had a reduction in executive functioning.[2-5]
The cognitive processes collectively referred to as executive functions are responsible for organizing, coordinating, and guiding goal-oriented behavior. Under the umbrella of executive functions, there are three domains: (1) Shifting, which includes task switching, attention, and dual-task processing; (2) updating, which involves updating working memory representations and processes; and (3) inhibition, which is related to taking decisions and involves inhibiting prevailing and automatic response. All three domains are linked with the fall risk in community-dwelling elderly.[6]
Cognitive decline associated with age or normal cognitive aging is a normal human phenomenon that varies from individual to individual. As we age, certain cognitive processes decline, associatively affecting other physiological functions of the human body. Due to progressive age, some cognitive processes face a major decline, while some may be much less affected. Mental functions such as verbal ability and general knowledge are less affected by aging as compared to other mental abilities such as memory, executive functions, processing speed, and reasoning. Each of these skills is necessary for carrying out daily tasks and living a self-reliant life. Some of the published literature suggested that cognitively impaired patients had poor balance and were more prone to falls.[6-8]
Physical and occupational therapists are among the health-care experts who frequently play a critical role in creating customized fall prevention strategies that can include cognitive training (CT) to reduce fall risk. According to Smith-Ray research, computer-based CT using straightforward games such as Road Tour, Jewel Diver, and Sweep Seeker enhanced visuospatial memory, processing speed, and inhibition. These improvements, in turn, enhanced balance and gait and reduced the risk of falls in elderly living in communities. Another study found that community-dwelling black older individuals who participated in a computer-based CT program under the guidance of a research assistant had better balance.[9,10]
A board game is any game where players place, rearrange, or remove pieces from a board designated with patterns that adhere to a predetermined game framework. Board games are a useful tool that can enhance participants’ comprehension, motivation, and cognitive performance. In a study conducted by Panphunpho et al., individuals who played board games showed improvement in cognitive processes (executive functions, memory, and attention) compared to the control group.[11,12] In the strategy-based board game Ludo, two to four players race to finish with their four tokens depending on the results of a single dice roll. It is a cross and circle game. Playing Ludo can improve strategic planning and decision-making abilities and enhance memory. It helps to develop an individual’s hands-on, reaction, thinking, and communication abilities. A study by Iizuka et al. proved that a board game similar to Ludo can be used to improve and maintain cognitive function.[13] The goal of the classic Chutes (Snakes and Ladders) game is to climb as high as you can without slipping down. Land on good deeds to ascend ladders. This game helps with an individual’s cognitive development and decision-making skills.[14]
The primary purpose of this study was to investigate the impact of implementing a CT program on balance and fall prevention among community-dwelling elderly. Specifically, the research aims to examine potential improvements in balance and the reduction of falls by implementing CT using simple board games. The overarching goal is to contribute to the existing literature by assessing whether a board game-based CT program conducted over eight weeks can enhance physical performance outcomes related to balance and walking in the older population.
By addressing this research question, the study seeks to establish whether the cognitive benefits derived from engaging in simple board games can translate into tangible improvements in the physical domain, particularly regarding balance and walking abilities among the elderly. If the association between board game-based CT and enhanced physical performance is supported, it could pave the way for such training to be considered an efficient approach to lower the incidence of falls in community-dwelling elderly. The underlying premise is that by improving an individual’s ability to navigate through their environment while effectively managing cognitive demands, a board game-based CT program may prove to be an accessible and effective strategy for fall prevention in the older population.
MATERIALS AND METHODS
Participants
It was a randomized control trial (Registered in clinical trial.gov with trial ID: NCT06047769). The research was conducted in Isra University Physiotherapy Clinic, Islamabad and Abid Hospital, Islamabad. The sample size was calculated using G-Power with effect size 0.4[9] alpha = 0.05 and power = 0.80 with a total number of participants of 64 and 32 in each group (experimental and control).
Both sexes with the age of 65 years or older with a mini-mental state examination (MMSE) score of 26 or above and a minimum of one self-reported fall in the previous two years or a Berg balance scale (BBS) score between more than 41 and <52 and those who agreed to devote the necessary amount of time as desired by the program. The study excluded participants with vertigo, neurological disorders, eye diseases, significant walking or balance impairments, and physical limitations that might hinder hand mobility, and those using psychotropic medicines.
Intervention
As an intervention, board games, including Ludo, chutes (snakes and ladders), and chess, were played at different intervals. A detailed intervention is described in Tables 1 and 2.
| Weeks | Intervention | Duration | Progression |
|---|---|---|---|
| Week 1–4 | Ludo | 30 min | No progression during this phase. |
| Chutes (snakes and ladders) | 15 min | ||
| Chess | 15 min | ||
| Week 5–8 | Ludo | 30 min | Multi-player mode will be added with each game except chess. |
| Chutes (snakes and ladders) | 15 min | ||
| Chess | 15 min |
| Weeks | Frequency and time duration of games | Experimental group | Control group |
|---|---|---|---|
| Week 0 (Baseline) | Pre-assessment+1 Week training of board games for experimental group | ||
| Weeks 1–4 | 3 times a week, 60 min/day. | Games including Ludo, Chutes (snakes and ladders), and Chess (Double player mode). | A complete control group with no intervention applied. |
| 4th week | Mid-assessment | ||
| Weeks 5–8 | 3 times a week, 60 min/day | Multiplayer mode games including Ludo, Chutes (snakes and ladders), except chess. | A complete control group with no intervention applied. |
| 8th week (final) | Post-assessment | ||
Outcome measure
BBS was used to assess balance and is considered a gold standard with high validity (0.93) and reliability (0.98) used to measure balance in the elderly.[15] MMSE, a collection of 11 questions to screen for cognitive impairment (difficulties with thinking, communicating, comprehending, and memory), frequently utilized by medical and other health-care professionals, has a reliability of (0.98) and validity (0.77).[16]
Dynamic gait index (DGI) is a clinical instrument to evaluate gait, balance, and fall risk, with a reliability of (0.98).[17] The timed up-and-go test (TUGT) is a quick and widely used clinical performance-based evaluation of lower limb function, mobility, and fall risk with a specificity of 0.70 and sensitivity of 0.57[18] and reliability of (0.98).[17]
Randomization
The participants were divided into two groups, experimental and control, through a sealed envelope approach, and the sampling strategy used was a non-probability convenient sampling technique.
Data collection procedure
After the approval, the assessment was done on the first day to screen and recruit participants and for baseline data (Pre-assessment). The participants in the experimental group received one week of training in board games; in the control group, those who played board games were asked to discontinue playing till the assessment of the eighth week. After four weeks, another data collection was performed to check the progress of individuals (Mid-assessment). At the end of treatment (after eight weeks), a post-assessment was conducted to check for the results of the given intervention. The CONSORT flow diagram is shown in Figure 1.
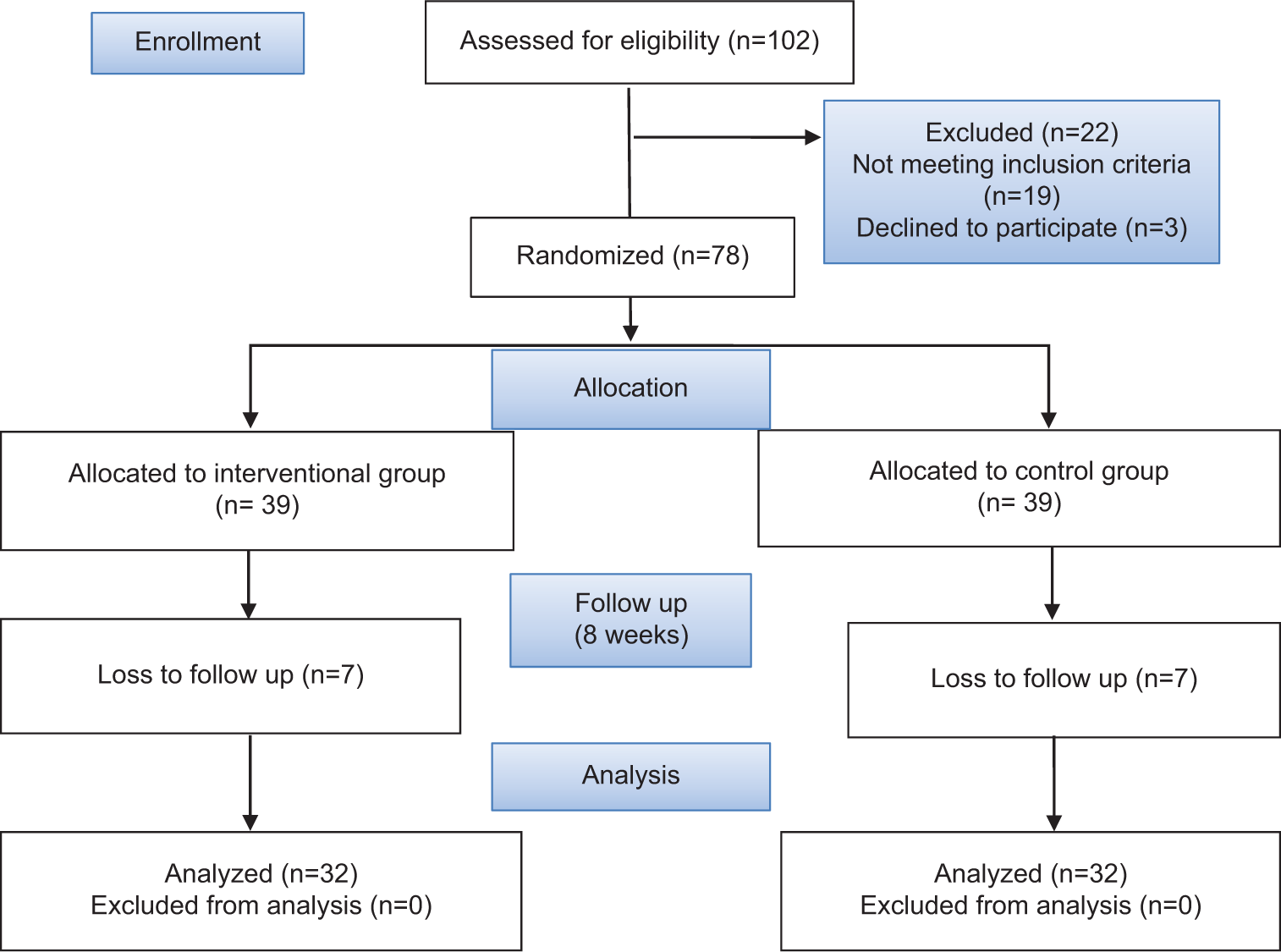
- Study consolidated standards of reporting trials (CONSORT) diagram.
Statistical analysis
Data was analyzed using the Statistical Package for the Social Sciences version 27. Data was analyzed descriptively by mean and median and demographic data was analyzed using frequency statistics. The normality of the data was analyzed through the Shapiro-Wilk Test. Data was analyzed using mixed and repeated measure analysis of variance (ANOVA). Partial Eta-squared values were reported as measures of effect size. The alpha value was 0.05.
RESULTS
The mean and standard deviation for the age of the control group were 67.91 ± 3.14 and that of the experimental group was 69.93 ± 4.77. Regarding sex, 16 males and 16 females were in the experimental group, while 15 males and 17 females were in the control group [Figure 2].
- Sex distribution.
A mixed-way ANOVA was conducted to investigate the impact of intervention and time on both groups. A significant main effect of time was seen within the groups at all three occasions with P ≤ 0.05 [Table 3].
| S. No. | Variables (n=64) | Experimental group | Control group | Box M | Both groups | Power | Error | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean±SD | Mean±SD | F (df) | η2 | P-value | |||||
| 1. | BBS | ||||||||
| Baseline | 47.25±1.85 | 48.37±2.24 | 86.623 | 7.932 (1.062) | 0.113 | 0.006** | 0.809 | 65.820 | |
| 4th week | 48.66±1.86 | 48.34±2.31 | |||||||
| 8th week | 49.84±5.15 | 48.06±2.77 | |||||||
| 2. | DGI | ||||||||
| Baseline | 19.65±1.45 | 20.41±1.60 | 5.460 | 69.323 (1.739) | 0.528 | 0.000*** | 1.000 | 107.817 | |
| 4th week | 20.34±1.58 | 20.47±1.54 | |||||||
| 8th week | 21.38±1.48 | 20.47±1.68 | |||||||
| 3. | MMSE | ||||||||
| Baseline | 26.87±0.83 | 27.41±0.87 | 5.680 | 93.676 (1.98) | 0.754 | 0.000*** | 1.000 | 61.000 | |
| 4th week | 27.69±0.93 | 27.31±0.93 | |||||||
| 8th week | 28.66±0.75 | 27.00±0.95 | |||||||
| 4. | TUGT | ||||||||
| Baseline | 10.40±0.69 | 10.26±0.73 | 3.615 | 13.481 (1.426) | 0.179 | 0.000*** | 0.986 | 88.382 | |
| 4th week | 10.38±0.69 | 10.24±0.73 | |||||||
| 8th week | 10.22±0.69 | 10.26±0.74 | |||||||
Level of significance:P<0.001*** and P<0.05**. BBS: Berg balance scale, DGI: Dynamic gait index, MMSE: Mini-mental state examination, TUGT: Timed up-and-go test, ANOVA: Analysis of variance, SD: Standard deviation, df: Degree of freedom, F: Variation between sample means/variation within the samples.
Repeated measure ANOVA was applied for within-group analysis. Balance was assessed using BBS, and the scores significantly improved from 47.2 ± 1.84 to 49.8 ± 5.15 with P < 0.05. Similarly, elder community dwellers were also analyzed for risk of falls; DGI scores also showed a significant improvement of mean scores from 19.65 ± 1.49 to 21.37 ± 1.47 (P < 0.05) in the experimental group. The results of MMSE showed significant improvement in cognition. The baseline readings were 26.8 ± 0.83, which improved to 28.6 ± 0.74 after eight weeks with P < 0.05. TUGT also showed a significant reduction in their scores, which were recorded as 10.40 ± 0.69 at baseline and 10.22 ± 0.67 after eight weeks, with P < 0.001. In the control group, community dwellers showed no significant improvement in balance. P-value came non-significant (P > 0.05) for BBS, DGI, and TUGT except MMSE (P < 0.05) [Table 4].
| S. No. | Variables | Experimental group | Control group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean diff. | Mean±SD | F (df) | η2 | P-value | Mean diff. | Mean±SD | F (df) | η2 | P-value | ||
| 1. | BBS | ||||||||||
| Baseline | −1.406 | 47.25±1.85 | 6.566 (1.044) | 0.175 | 0.014** | 0.031 | 48.37±2.24 | 3.131 (1.565) | 0.092 | 0.064 | |
| 4th week | −1.188 | 48.66±1.86 | 0.281 | 48.34±2.31 | |||||||
| 8th week | −2.594 | 49.84±5.15 | 0.313 | 48.06±2.77 | |||||||
| 2. | DGI | ||||||||||
| Baseline | −0.688 | 19.65±1.45 | 146.95 (1.916) | 0.826 | 0.000*** | −0.063 | 20.41±1.60 | 0.261 (1.734) | 0.008 | 0.729 | |
| 4th week | −1.031 | 20.34±1.58 | 0.000 | 20.47±1.54 | |||||||
| 8th week | −1.719 | 21.38±1.48 | −0.063 | 20.47±1.68 | |||||||
| 3. | MMSE | ||||||||||
| Baseline | −0.813 | 26.87±0.83 | 161.48 (1.947) | 0.839 | 0.000*** | 0.094 | 27.41±0.87 | 6.851 (1.931) | 0.181 | 0.002** | |
| 4th week | −0.969 | 27.69±0.93 | 0.313 | 27.31±0.93 | |||||||
| 8th week | −1.781 | 28.66±0.75 | 0.406 | 27.00±0.95 | |||||||
| 4. | TUGT | ||||||||||
| Baseline | 0.093 | 10.40±0.69 | 28.427 (1.377) | 0.478 | 0.000*** | 0.021 | 10.26±0.73 | 0.407 (1.413) | 0.013 | 0.597 | |
| 4th week | 0.086 | 10.38±0.69 | −0.016 | 10.24±0.73 | |||||||
| 8th week | 0.179 | 10.22±0.69 | 0.004 | 10.26±0.74 | |||||||
Level of significance:P<0.001***and P<0.05**. BBS: Berg balance scale, DGI: Dynamic gait index, MMSE: Mini-mental state examination, TUGT: Timed up-and-go test, ANOVA: Analysis of variance, SD: Standard deviation, df: Degree of freedom, F: Variation between sample means/variation within the samples.
One-way ANOVA was applied to the group analysis, including the experimental and control groups. For BBS, at baseline, the F-value was 4.801 with P < 0.05, showing a significant difference between the groups. In the fourth week, the F-value was 0.356 with P > 0.05, and in the eighth week, the F-value was 2.969 with P > 0.05, both occasions showing a non-significant difference between the groups.
BBS (baseline) (4.801 [1, 0.264] = 0.032, P < 0.05), BBS (Week 4) (0.356 [1, 0.260] = 0.553, P > 0.05), and BBS (Week 8) (2.969 [1, 0.525] = 0.090, P > 0.05) [Table 5].
| Variable | Mean±SD | F | df | η2 | P-value |
|---|---|---|---|---|---|
| BBS at baseline | |||||
| Experimental group | 47.25±1.85 | 4.801 | 1 | 0.072 | 0.032** |
| Control group | 48.37±2.24 | ||||
| BBS in 4th week | |||||
| Experimental group | 48.65±1.86 | 0.356 | 1 | 0.006 | 0.553 |
| Control group | 48.34±2.31 | ||||
| BBS in 8th week | |||||
| Experimental group | 49.84±5.15 | 2.969 | 1 | 0.046 | 0.090 |
| Control group | 48.06±2.77 |
Level of significance:P<0.05**. BBS: Berg balance scale, ANOVA: Analysis of variance, SD: Standard deviation, df: Degree of freedom, F: Variation between sample means/variation within the samples.
For variable DGI, at baseline, the F-value was 3.747 with P > 0.05, showing a non-significant difference between the groups. In the fourth week, the F-value was 0.103, with P > 0.05, showing a non-significant difference between the groups and in the eighth week, it was 5.240, with P < 0.05, showing a significant difference between the groups.
DGI (baseline) (3.747 [1, 0.198] = 0.058, P > 0.05), DGI (Week 4) (0.103 [1, 0.194] = 0.750, P > 0.05), and DGI (Week 8) (5.240 [1, 0.204] = 0.025, P < 0.05) [Table 6].
| Variable | Mean±SD | F | df | η2 | P-value |
|---|---|---|---|---|---|
| DGI at baseline | |||||
| Experimental group | 19.65±1.49 | 3.747 | 1 | 0.057 | 0.058 |
| Control group | 20.40±1.60 | ||||
| DGI at 4th week | |||||
| Experimental group | 20.34±1.58 | 0.103 | 1 | 0.002 | 0.750 |
| Control group | 20.46±1.54 | ||||
| DGI at 8th week | |||||
| Experimental group | 21.37±1.47 | 5.240 | 1 | 0.078 | 0.025** |
| Control group | 20.46±1.68 |
Level of significance: P<0.05**. DGI: Dynamic gait index, ANOVA: Analysis of variance, SD: Standard deviation, df: Degree of freedom, F: Variation between sample means/variation within the samples.
At baseline, the F-value was 6.191 for variable MMSE with P < 0.05, showing a significant difference between the groups. In the fourth week, the F-value was 5.595, having P > 0.05, showing a non-significant difference between the groups and in the eighth week was 60.179, with P < 0.05, showing a significant difference.
MMSE (baseline) (6.191 [1, 0.111] = 0.016, P < 0.05), MMSE (Week 4) (5.595 [1, 0.118] = 0.112, P > 0.05), and MMSE (Week 8) (60.179 [1, 0.149] = 0.000, P < 0.05) [Table 7].
| Variable | Mean±SD | F | df | η2 | P-value | |
|---|---|---|---|---|---|---|
| MMSE at baseline | ||||||
| Experimental group | 26.87±0.83 | 6.191 | 1 | 0.091 | 0.016** | |
| Control group | 27.40±0.87 | |||||
| MMSE at 4th week | ||||||
| Experimental group | 27.68±0.93 | 5.595 | 1 | 0.040 | 0.112 | |
| Control group | 27.31±0.93 | |||||
| MMSE at 8th week | ||||||
| Experimental group | 28.65±0.74 | 60.179 | 1 | 0.493 | 0.000*** | |
| Control group | 27.00±0.95 |
Level of significance:P<0.001*** and P<0.05**. MMSE: Mini-mental state examination, ANOVA: Analysis of variance, SD: Standard deviation, df: Degree of freedom, F: Variation between sample means/variation within the samples.
For variable TUGT, at baseline, the F-value was 0.594, with P > 0.05, showing a non-significant difference between the groups. In the fourth week, the F-value was 0.134, and in the eighth week, it was 0.044, both having P > 0.05, showing a non-significant difference between the groups.
TUGT (baseline) (0.594 [1, 0.089] = 0.444, P > 0.05), TUGT (Week 4) (0.134 [1, 0.088] = 0.715, P > 0.05), and TUGT (Week 8) (0.044 [1, 0.088] = 0.834, P > 0.05) [Table 8].
| Variable | Mean±SD | F | df | η2 | P-value |
|---|---|---|---|---|---|
| TUGT at baseline | |||||
| Experimental group | 10.40±0.69 | 0.594 | 1 | 0.009 | 0.444 |
| Control group | 10.26±0.73 | ||||
| TUGT at 4th week | |||||
| Experimental group | 10.31±0.68 | 0.134 | 1 | 0.002 | 0.715 |
| Control group | 10.24±0.73 | ||||
| TUGT at 8th week | |||||
| Experimental group | 10.22±0.68 | 0.044 | 1 | 0.001 | 0.834 |
| Control group | 10.26±0.63 |
DISCUSSION
This study was carried out to determine the effects of board games on cognition, balance, and fall risk with a hypothesis that there would be no difference in cognition, balance, and fall risk of community-dwelling older individuals when compared to the group who played board games and the control group who did not play board games. To see the effects of board games on balance and cognition in older community individuals, the results showed significant improvement of cognition on MMSE, BBS, and DGI after eight weeks of training in the elders who played board games. Other than that, the experimental group significantly reduced their TUGT scores. Similarly, in this study, the analysis showed a significant difference between the experimental group and control group for MMSE (P <0.001), BBS (P < 0.001), DGI (P <0.001), and TUGT (P < 0.001).
This study showed that an 8-week CT program by playing board games reduced the risk of falls and enhanced cognitive function. The current results are consistent with a prior study that showed improvement in older individuals’ response times and postural sway following their involvement in a board game-based training program.[19] One aspect of the executive function is the ability to split attention, which was demonstrated by a quicker TUGT time during the verbal fluency task. This result is in line with other research that showed how enhancing older individuals’ capacity to multitask may be achieved by concurrent physical and CT.[19,20] The previous studies (Dartigues et al. and Verghese et al.) have demonstrated that playing board games can enhance cognitive abilities in people who are healthy elderly.[21,22]
Similar to our study, the life-size board game intervention, which was centered on physical activity, seemed to have improved the ambulation of nursing home patients, according to research by Mouton et al. Moreover, it was also concluded that BBS and DGI scores were seen to improve in the experimental group receiving physical training along with board games for up to eight weeks.[23]
Brain training using games will promote neuroplasticity, build cognitive reserve, and boost brain size, all of which will help to preserve or enhance cognitive function.[24] Perhaps due to the fact that game-based CT may control cognitive performance by building neural scaffolding and boosting neural activity.[25] According to Zhang and Kaufman (2016), the scaffolding hypothesis of aging and cognition describes scaffolding as the insertion of new circuitry to sustain brain activity that has become inefficient, noisy, or both.[26] By regularly exposing an individual to novel training activities and situations, brain training can enhance and facilitate the growth of compensatory mechanisms, thereby averting cognitive decline.[25]
In the present study, whether the improvement seen in the experimental group has a retention effect is uncertain. Given these methodological constraints, longer-term follow-up investigations are necessary to validate the research results. Second, although the results showed statistically significant improvements for TUGT, MMSE, DGI, and BBS, it was impossible to interpret these improvements or determine whether they were the result of measurement error or the training’s clinically meaningful benefit. Last but not least, the study’s subjects were relatively healthy. Thus, its conclusions might not apply to the elderly with neurological impairment.
CONCLUSION
The present study showed that an eight-week interactive physical-CT program based on board games improved cognitive function, reduced fall risk by improving physiological fall risk factors such as body sway and speed processing, and enhanced global cognitive performance by enhancing dual-task performance. The interactive board game-based physical-CT program was also useful for older individuals who live in the community by improving mobility and balance.
Recommendations
Longer-term follow-up investigations on frail elders are necessary to validate the research results. Board games other than Ludo, Chutes (snakes and ladders), and Chess should be considered in future research for balance improvement. Furthermore, the data on the smallest real difference and minimal clinically important difference for these outcome measures should be available in future studies.
ACKNOWLEDGMENT
The authors would like special appreciation to the supervisor for providing appropriate direction and support throughout the research process.
AUTHORS’ CONTRIBUTIONS
MA contributed to the conception, study design, and data collection and is responsible for the manuscript’s content and similarity index. IA and MS contributed to study conception, data analysis, and interpretation. OSAG contributed to article drafting, proofreading, and revisions. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
ETHICAL APPROVAL
The research/study approved by the Institutional Review Board at Riphah International University Islamabad, number Ref#Riphah/RCRS/REC/01539, dated May 17, 2023.
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
USE OF ARTIFICIAL INTELLIGENCE (AI)-ASSISTED TECHNOLOGY FOR MANUSCRIPT PREPARATION
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Psychiatric morbidity in geriatric population in old age homes and community: A comparative study. Indian J Psychol Med. 2012;34:39-43.
- [CrossRef] [PubMed] [Google Scholar]
- The geriatric patient: A systematic approach to maintaining health. Am Fam Physician. 2000;61:1089-104.
- [Google Scholar]
- The state, society, and foreign capital in India. In: Cambridge. UK: Cambridge University Press; 2018.
- [CrossRef] [Google Scholar]
- Health and needs assessment of geriatric patients: Results of a survey at a teaching hospital in Karachi. J Pak Med Assoc. 2006;56:470-4.
- [Google Scholar]
- Effect of cognitive function on balance and posture control after stroke. Neural Plast. 2021;2021:6636999.
- [CrossRef] [PubMed] [Google Scholar]
- Hearing loss and cognitive decline in older adults. JAMA Intern Med. 2013;173:293-9.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of cognitive training on balance and gait in older adults. J Gerontol B Psychol Sci Soc Sci. 2015;70:357-66.
- [CrossRef] [PubMed] [Google Scholar]
- A randomized trial to measure the impact of a community-based cognitive training intervention on balance and gait in cognitively intact black older adults. Health Educ Behav. 2014;41(1_suppl):62S-9.
- [CrossRef] [PubMed] [Google Scholar]
- The effectiveness of intervention with board games: A systematic review. BioPsychoSocial Med. 2019;13:22.
- [CrossRef] [PubMed] [Google Scholar]
- Positive effects of Ska game practice on cognitive function among older adults. J Med Assoc Thai. 2013;96:358-64.
- [Google Scholar]
- Pilot randomized controlled trial of the GO game intervention on cognitive function. Am J Alzheimers Dis Other Demen. 2018;33:192-8.
- [CrossRef] [PubMed] [Google Scholar]
- Humanities, Snake and ladder games in cognition development on students with learning difficulties. Rev Arts Humanit. 2014;3:217-29.
- [Google Scholar]
- Reliability and validity of the Turkish version of the Berg Balance Scale. J Geriatr Phys Ther. 2008;31:32-7.
- [CrossRef] [PubMed] [Google Scholar]
- The mini mental state examination: Review of cutoff points adjusted for schooling in a large Southern Brazilian sample. Dement Neuropsychol. 2010;4:35-41.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability, validity, and responsiveness of three scales for measuring balance in patients with chronic stroke. BMC Neurol. 2018;18:141.
- [CrossRef] [PubMed] [Google Scholar]
- The prognostic validity of the timed up and go test with a dual task for predicting the risk of falls in the elderly. Gerontol Geriatr Med. 2016;2:2333721416637798.
- [CrossRef] [PubMed] [Google Scholar]
- A randomized controlled pilot study of home-based step training in older people using videogame technology. PLoS One. 2013;8:e57734.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of simultaneously performed cognitive and physical training in older adults. BMC Neurosci. 2013;14:103.
- [CrossRef] [PubMed] [Google Scholar]
- Playing board games, cognitive decline and dementia: A French population-based cohort study. BMJ Open. 2013;3:e002998.
- [CrossRef] [PubMed] [Google Scholar]
- Leisure activities and the risk of dementia in the elderly. N Engl J Med. 2003;348:2508-16.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of a giant exercising board game intervention on ambulatory physical activity among nursing home residents: A preliminary study. Clin Interv Aging. 2017;12:847-58.
- [CrossRef] [PubMed] [Google Scholar]
- Hippocampal plasticity underpins long-term cognitive gains from resistance exercise in MCI. Neuroimage Clin. 2020;25:102182.
- [CrossRef] [PubMed] [Google Scholar]
- The Synapse project: Engagement in mentally challenging activities enhances neural efficiency. Restor Neurol Neurosci. 2015;33:865-82.
- [CrossRef] [PubMed] [Google Scholar]
- Physical and cognitive impacts of digital games on older adults: A meta-analytic review. J Appl Gerontol. 2016;35:1189-210.
- [CrossRef] [PubMed] [Google Scholar]




