Translate this page into:
Factors associated with fear of re-injury in physically active individuals after an anterior cruciate ligament reconstruction
2 College of Medicine, King Saud Bin Abdulaziz University for Health Sciences; King Abdullah International Medical Research Center; Department of Surgery, Orthopedic Division, Ministry of the National Guard-Health Affairs, Jeddah, Saudi Arabia
Corresponding Author:
Osama Khojah
King Saud Bin Abdulaziz University for Health Sciences, COM-WR, Makkah
Saudi Arabia
osamakhojah001@gmail.com
| How to cite this article: Alswat M, Khojah O, Dabroom A, Alghamdi A, Alshibely A, Algarni H, Almadani M, Alswat A, Alshehri M. Factors associated with fear of re-injury in physically active individuals after an anterior cruciate ligament reconstruction. J Musculoskelet Surg Res 2021;5:30-34 |
Abstract
Objectives: Fear of re-injury is a psychological consequence of an anterior cruciate ligament (ACL) injury. For physically active individuals, fear of re-injury is a frequent cause for not returning to their preinjury physical activity level after ACL reconstruction. The aim of this study is to investigate fear of re-injury, and factors associated with its increase in physically active individuals who had an ACL reconstruction. Methods: A cross-sectional study was conducted in our institute. An online survey was sent to participants. The survey focused on sports participation and included two instruments, the International Knee Documentation Committee (IKDC) and an 11-item version of the Tampa Scale for Kinesiophobia (TSK-11). Results: In total, 103 individuals participated in this study. The mean age was 35 years, males constituted 98% and the mean body mass index (BMI) was 27.8 kg/m2. The mean post-surgery follow-up period was 5.1 years, and around 59.2% of the sample returned to sports. Soccer was the most frequent (73.8%) sport practiced. The mean TSK-11 was 27.9. Age, BMI, concomitant knee injury, time from injury to surgery, follow-up period, and sport type were not correlated with fear of re-injury. However, sports participation frequency, returning to sports, and IKDC scores were significantly correlated with fear of re-injury. Conclusion: Fear of re-injury after an ACL reconstruction is affected by the frequency of sports participation, resuming activity after injury and knee function. Optimizing these factors may improve the psychological outcomes after an ACL reconstruction.
Introduction
Injury to the anterior cruciate ligament (ACL) is a major orthopedic sport-related injury, especially in individuals participating in sports with twisting, pivoting, and cutting movements.[1],[2],[3] The incidence of ACL injury ranges from 100,000 to 200,000 injuries annually in the United States alone. ACL tears are managed with ACL reconstruction surgery, which has short- and long-term goals.[3],[4] The short-term goals are to restore the stability and function of the knee, and ultimately return to full preinjury level of activity.[4] The restoration also focuses on preventing future meniscal tears or cartilage defects.[3] The long-term goal of the surgery is to prevent posttraumatic arthritis.[4]
The estimated timeframe for athletes to return to sports after the ACL rehabilitation protocol is about 1 year. However, a goal only two-thirds of the athletes achieve.[2],[3] According to Chmielewski et al., only 20%–50% of the patients who completed the ACL rehabilitation protocol returned to the same sport after surgery, and 10%–70% resumed their preinjury sport but at a reduced activity level or with functional impairment.[5] There are several hypotheses regarding the factors that contribute to not returning to sports. For example, the ACL rehabilitation programs' lack coherence or delaying returning to sports unless the patient meets the strength and function targets.[6]
An ACL injury has a significant psychological impact on athletes, inhibiting the rehabilitation process, and delaying the return to sports.[1] These factors have been reported extensively in sports literature. According to Christino et al. and Chao-Jung et al., injured athletes are prone to have an unpleasant experience. Mood disturbances and disorders, ranging from low self-esteem to depression.[1] In addition, adolescent athletes tend to experience psychological distress and post-traumatic stress disorders, which may cause poor coping responses.[1] These reactions occur more frequently directly after the injury, and decrease as the patients undergoes rehabilitation, but may recur before the return to sports.[1],[6] Fear of re-injury or kinesiophobia is a frequent psychological response to a sport-related injury.[6] Several studies reported that fear is a major cause for nonreturning to sports.[2],[5] A systematic review and meta-analysis, by Ardern et al., investigated the postoperative return to sports after an ACL injury, included 12 studies reporting the level of sports participation changes, and it showed that fear of re-injury prevented 19% of the patients from returning to preinjury levels.[7]
The aim of this study was to assess fear of re-injury after ACL reconstruction and identify factors and variables associated with its increase.
Subjects and Methods
This study was conducted at the Orthopedic Department, King Abdulaziz Medical City in Jeddah (KAMC-J), Saudi Arabia. A cross-sectional design was used. After reviewing the electronic hospital records from January 2011 to December 2018, a consecutive sampling technique was used. There were 553 patients who had ACL reconstruction surgery. They were contacted with a mobile message, which included an invitation to participate in an online survey. Reminder messages were sent between 3 days and 1 week after the first message. Of the 553 patients, 117 agreed to participate and completed the survey, a response rate of 21%. Out of 117 participants, 103 fulfilled the inclusion criteria. Those who fulfilled the following inclusion criteria were included; age from 18 to 50 years, have a unilateral knee injury, and participated in sports regularly before the ACL reconstruction surgery.
Demographic information including gender, age, body mass index (BMI) at the time of filling the questionnaires, marital status, and employment status were collected. The injury history consisted of the side of the injury, time from injury to ACL reconstruction, concomitant knee injuries such as meniscal or other ligamentous injuries, time from ACL reconstruction to follow-up, and the number of visits before surgery were all collected.
Sports participation included the frequency of participating in sports per week, the type of sports, as well as the resumption of sporting activities after the ACL reconstruction surgery.
Knee function was assessed using an Arabic version of the International Knee Documentation Committee's subjective knee evaluation form (IKDC), which was translated by Ahmed et al. and shown to be valid and reliable for the Arabic-speaking population.[8] The IKDC is widely accepted and used in the assessment of patients with an ACL injury.[9] It contains three fields, including knee symptoms, sports activities, and function. The score ranges from 0 to 100, with higher scores demonstrating better knee function.
To assess the participants' level of fear of movement and re-injury, the Tampa Scale for Kinesiophobia (TSK) was used. The TSK, designed in 1991 by Miller et al., is one of the first tools to assess fear related to pain. It is a self-report questionnaire composed of 17 statements, rated on a 4-point Likert scale.[10] In 2005, Woby et al. proposed the TSK-11, a shorter version containing 11 items.[11] The TSK-11 is a valid and reliable psychometric measurement for kinesiophobia and re-injury in several musculoskeletal disorders such as low back pain, fibromyalgia, and sports injury.[12] The total TSK-11 score ranges from 11 to 44 points, and a higher TSK-11 scores indicate higher fear of movement or re-injury.[11] A translated Arabic version by Juweid et al. was used.[13]
Statistical analyses were performed using IBM Statistical Software for Social Sciences (SPSS) for Windows, version 25 (IBM Corp., Armonk, N. Y., USA). Continuous variables are described as mean ± standard deviation (SD). Categorical variables are summarized using descriptive statistics such as frequency and percentage. After examining all variables for normality, a Pearson correlation, Student's t-test, and ANOVA test were used to determine the association between the dependent and independent variables. A P < 0.01 was considered statistically significant.
Results
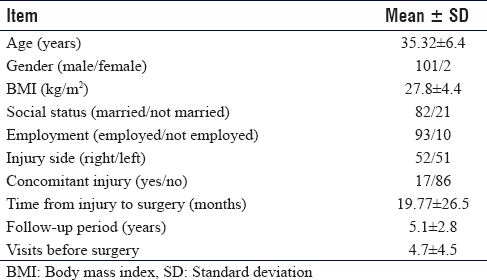
A total of 103 participants fulfilled the inclusion criteria with a male majority (98%). The mean age was 35.32 ± 6.4 years and the mean BMI, 27.8 ± 4.4 kg/m2. Regarding social status, the majority were married (79.6%) and employed (90.3%). Almost half (50.5%) injured the right knee, and 83.3% had no concomitant knee injury. The mean time from injury to surgery was 19.77 ± 26.5 months and the mean post-surgery follow-up period was 5.1 ± 2.8 years. The mean number of clinic visits before the date of surgery and after the injury was 4.7 ± 4.5 visits. Demographic details are shown in [Table - 1].
![[Table - 1]](#tbl_SaudiOrthopJ_2021_5_1_30_309269_t1.jpg){kind=link}
Sport participation and return
Soccer was the preferred sport (73.8%). Other sports included jogging and running (14.6%), volleyball (5.8%), weightlifting (1%), and other sports (4.9%). The frequency of sports activities per week was 4.5 ± 2.2 times. In terms of the resumption of participation, just more than half (59.2%) resumed their sporting activities. At the time of inclusion, the sample's mean IKDC score was 59.8 ± 18.3.
TSK score and relations to other factors
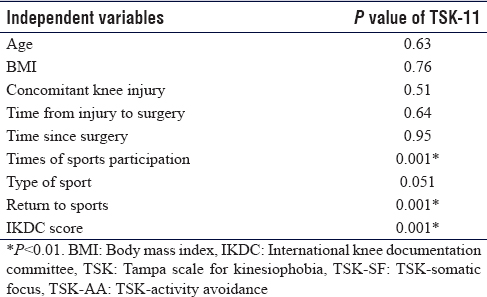
The mean TSK-11 score was 27.97 ± 8. Age, BMI, follow-up after surgery, and time from injury to surgery were not significantly correlated with TSK-11 when using a Pearson's correlation. On the other hand, as the frequency of participating in sports per week before injury increased, TSK-11 significantly increased (r (95) = 0.36, P < 0.001), 7 participants did not specify their sports participation. Regarding the concomitant knee injury, there was no significant difference in the mean score of the groups with and without an injury. Regarding the type of sport, using the ANOVA to compare the scores of participants playing different types of sports, participation in volleyball scored higher than the others. However, the difference was not significant (P = 0.051). Regarding resuming sporting activities, the group resuming sporting activities scored a mean of 25.6 ± 8 in TSK-11, which was significantly lower (P < 0.001) than the group who did not resume activities, whose mean score was 31.4 ± 6.7. A significant correlation was found between the IKDC score and TSK-11 (r (102) = −0.47, P < 0.001) score, as the knee function was higher when the fear of re-injury was lower. Details on variables' significance are shown in [Table - 2].
![[Table - 2]](#tbl_SaudiOrthopJ_2021_5_1_30_309269_t2.jpg){kind=link}
Discussion
Reducing fear of re-injury is an important goal of rehabilitation because it helps regain a high level of function, which is the main goal for almost all patients.[5] In terms of the demographic information of the sample, the high proportion of males is attributed to the cultural norms in Saudi Arabia at the time of the surgeries, precluding women from participating in sports in public places. In our study, age was not significantly associated with the total TSK. Older individuals have a decreased perception of their physical capabilities, supported by Ross et al., who reported “getting older” as a cause for not resuming their pre-injury level of sports. The authors also reported that older male athletes generally had an increased fear of re-injury.[2] Lentz et al. found that the group who did not return to sports due to a fear of re-injury, was significantly older than the counter group, with a mean age of 29.7 and 21 years, respectively (P = 0.004).[13] However, Hart et al. reported that in a group with osteoarthritis (OA), older age had a significant correlation with a higher TSK score (r = −0.289; P = 0.049).[14] No significant differences in fear of re-injury were found between the other demographic variables.[13] In regards to BMI, there was no significant correlation with the total TSK-11. However, in a study conducted by Vincent et al., 31.3% of the patients with a knee pain-related diagnosis had ACL reconstruction-related causes.[15] They also reported that the morbidly obese group scored significantly higher on the TSK than the non-obese group (P = 0.007).[15] Consequently, weight reduction should be an important strategy in the management and rehabilitation programs. Patients with ACL tears frequently suffer concomitant knee injuries due to the nature of the injury mechanisms. In the current study, 16.7% of the sample had a concomitant knee injury. In a study by Figueiredo et al., the most frequently reported associated injuries, included lesions in the medial meniscus, followed by the lateral meniscus and to a lesser degree, subchondral lesions.[16] We have not observed significant differences between patients with and without other knee injuries in the context of the TSK. In contrast, Hart et al. observed a significant increase of fear of re-injury in groups that suffered from OA compared to the group without OA.[17] It is plausible that the fear of re-injury could be increased in those affected by OA.
The inability to resume sporting activities after an ACL reconstruction is mainly attributed to fear of re-injury. In the current study, just more than half (59.2%) resumed sporting activities, which is lower than what was reported by Bauer et al.[18] The difference may be due to the other studies, included athletes, whether amateur or professional, whereas the current study included a sample, which did not target athletes exclusively. The most frequent cause for not resuming sports is fear of re-injury, as reported in the meta-analysis done by Ardern et al.[7] In the current study, a significant relationship was found between resuming sports participation and the degree of fear of re-injury. The group that did not resume sporting activities scored higher on the TSK-11. The finding is supported by Kvist et al., who reported that participants, who did not return to their preinjury sport level, had a higher degree of fear of re-injury than their counterparts.[19] It is possible to infer that psychological counseling and management will decrease fear of re-injury, increase functionality and facilitate participating in sports. The mean time from injury to surgery was not contributing to fear of movement or re-injury, and it was not statistically significant with the TSK score. Chmielewski et al. also reported no significant relationship between the time to surgery and the three groups that were included in their study.[5] The findings suggest patients are less concerned when returning to sports post ACL reconstruction if they experience fewer episodes of instability and giving way, due to the reduced use of the affected knee. This leads to patients returning to sports participation post ACL reconstruction with fewer concerns. However, Ardern et al. found that the participants who had their surgery <3 months after the injury had significantly lower fear of re-injury, compared with participants who had surgery after 3 months from the time of injury.[3] It may be inferred that a shorter preoperative period possibly will result in fewer episodes of giving away and a shorter duration of knee dysfunctionality, which may reduce the detrimental effect on the patient's mentality. Concerning the type of sports, playing volleyball scored higher than the other types of sports. The nature of volleyball relies heavily on jumping, landing, and high-speed direction changes, which increases the likelihood of knee instability resulting in a fear of re-injury. Environmental conditions such as playing surfaces were a significant (P < 0.05) concern for the female group in the Ardern et al. study.[3] It was presumed that due to particular netball demands, the quality of the playing surface might result in fear of re-injury.[3] The differences in the results are explained by the varying sports played in countries and the specific demands of each sport. Surprisingly, subjects who reported higher sports participation frequencies also had significantly higher TSK-11 scores. We hypothesize that it might be due to psychological factors such as high awareness and expectation of the sport's demands. Fully comprehending what it takes to return to sports might present a sense of fear, which might not be found in those who do not participate in sports as much. However, further research is definitely needed to prove or refute this hypothesis. There was no significant relationship between follow-up after surgery and TSK-11 score. Similarly, Ardern et al. found no difference in fear of re-injury between patients who were followed up before and after 4 years' post-operation.[3] Chmielewski et al. emphasized the importance of managing the patient's fear during the rehabilitation process post ACL reconstruction to reduce the effect on the subjective knee function at the time of resuming sports.[5],[14] The IKDC score in our study was significantly correlated with the fear of re-injury. This was supported by two studies that reported a correlation between subjective knee function and fear of re-injury.[19],[20]
This study has a number of limitations. The first is the use of a self-administered questionnaire, which may have affected the accuracy. In addition, the study had a small sample size, with a low response rate. The acknowledged gender discrepancy prevents the applicability of the findings to other societies.
Conclusion
Fear of re-injury is one of the most important psychological aspects of ACL tear management. We have reported multiple factors that could increase fear of re-injury despite normal knee function, like the frequency of sports participation, resuming activity after injury, and knee function.
Recommendations
Based on our findings, we recommend implementing individualized strategies to support each patient's psychological needs, to consider the type of sports practiced, especially high-risk sport, to promote and encourage physical activity and participation in sports to overcome the fear barrier and decrease fear of re-injury, and to providing psychological support to the patients in the postoperative period.
Ethical considerations
This study was approved by the Institutional Review Board at King Abdullah International Medical Research Centre with reference number: JED-19-427780-149292 obtained on September 25, 2019. The informed consent included instructions related to the completion and submission of the survey. Participation in the study was explained to participants in the invitation link for the online questionnaire and their completion and submission of the questionnaire was considered as consent for participation. The data were only accessible to the authors and was password protected. Information that might identify the patients, such as names and medical record numbers (MRNs), were not collected. A serial number was given to the patients in place of the MRNs. By participating in the questionnaire, patients consented to be part of the study and agreed for the publications of the results.
Financial support and sponsorship
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
There are no conflicts of interest.
Author's contribution
MMA and OMK were responsible for the conception and design of the study. MMA and AHA provided statistical expertise and managed the analysis and interpretation of the data. All authors participated in drafting the article. All authors provided critical revision of the article for important intellectual content. AMA, AHA, MSA, AYA, AAD, and OMK participated in collecting and assembling the data. All authors have critically reviewed and approved the final draft and are responsible for the manuscript's content and similarity index.
| 1. | Christino MA, Fantry AJ, Vopat BG. Psychological aspects of recovery following anterior cruciate ligament reconstruction. J Am Acad Orthop Surg 2015;23:501-9. [Google Scholar] |
| 2. | Ross CA, Clifford A, Louw QA. Factors informing fear of reinjury after anterior cruciate ligament reconstruction. Physiother Theory Pract 2017;33:103-14. [Google Scholar] |
| 3. | Ardern CL, Taylor NF, Feller JA, Webster KE. Fear of re-injury in people who have returned to sport following anterior cruciate ligament reconstruction surgery. J Sci Med Sport 2012;15:488-95. [Google Scholar] |
| 4. | Flanigan DC, Everhart JS, Pedroza A, Smith T, Kaeding CC. Fear of reinjury (kinesiophobia) and persistent knee symptoms are common factors for lack of return to sport after anterior cruciate ligament reconstruction. Arthroscopy 2013;29:1322-9. [Google Scholar] |
| 5. | Chmielewski TL, Jones D, Day T, Tillman SM, Lentz TA, George SZ. The association of pain and fear of movement/reinjury with function during anterior cruciate ligament reconstruction rehabilitation. J Orthop Sports Phys Ther 2008;38:746-53. [Google Scholar] |
| 6. | Hsu CJ, Meierbachtol A, George SZ, Chmielewski TL. Fear of reinjury in athletes. Sports Health 2017;9:162-7. [Google Scholar] |
| 7. | Ardern CL, Webster KE, Taylor NF, Feller JA. Return to sport following anterior cruciate ligament reconstruction surgery: A systematic review and meta-analysis of the state of play. Br J Sports Med 2011;45:596-606. [Google Scholar] |
| 8. | Ahmed KM, Said HG, Ramadan EKA, Abd El-Radi M, El-Assal MA. Arabic translation and validation of three knee scores, Lysholm Knee Score (LKS), Oxford Knee Score (OKS), and International Knee Documentation Committee Subjective Knee Form (IKDC). SICOT J 2019;5:6. [Google Scholar] |
| 9. | Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res (Hoboken) 2011;63 Suppl 11:S208-28. [Google Scholar] |
| 10. | Hudes K. The Tampa Scale of Kinesiophobia and neck pain, disability and range of motion: A narrative review of the literature. J Can Chiropr Assoc 2011;55:222-32. [Google Scholar] |
| 11. | Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: A shortened version of the Tampa Scale for Kinesiophobia. Pain 2005;117:137-44. [Google Scholar] |
| 12. | George SZ, Lentz TA, Zeppieri G, Lee D, Chmielewski TL. Analysis of shortened versions of the Tampa Scale for Kinesiophobia and pain catastrophizing scale for patients after anterior cruciate ligament reconstruction. Clin J Pain 2012;28:73-80. [Google Scholar] |
| 13. | Lentz TA, Zeppieri G Jr., George SZ, Tillman SM, Moser MW, Farmer KW, et al. Comparison of physical impairment, functional, and psychosocial measures based on fear of reinjury/lack of confidence and return-to-sport status after ACL reconstruction. Am J Sports Med 2015;43:345-53. [Google Scholar] |
| 14. | Chmielewski TL, Zeppieri G Jr., Lentz TA, Tillman SM, Moser MW, Indelicato PA, et al.: Longitudinal changes in psychosocial factors and their association with knee pain and function after anterior cruciate ligament reconstruction. Phys Ther 2011;91:1355-66. [Google Scholar] |
| 15. | Vincent HK, Lamb KM, Day TI, Tillman SM, Vincent KR, George SZ. Morbid obesity is associated with fear of movement and lower quality of life in patients with knee pain-related diagnoses. PM R 2010;2:713-22. [Google Scholar] |
| 16. | Brophy RH, Zeltser D, Wright RW, Flanigan D. Anterior cruciate ligament reconstruction and concomitant articular cartilage injury: Incidence and treatment. Arthroscopy 2010;26:112-20. [Google Scholar] |
| 17. | Hart HF, Collins NJ, Ackland DC, Crossley KM. Is impaired knee confidence related to worse kinesiophobia, symptoms, and physical function in people with knee osteoarthritis after anterior cruciate ligament reconstruction? J Sci Med Sport 2015;18:512-7. [Google Scholar] |
| 18. | Bauer M, Feeley BT, Wawrzyniak JR, Pinkowsky G, Gallo RA: Factors affecting return to play after anterior cruciate ligament reconstruction: A review of the current literature. Phys Sportsmed 2014;42:71-9. [Google Scholar] |
| 19. | Kvist J, Ek A, Sporrstedt K, Good L. Fear of re-injury: A hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2005;13:393-7. [Google Scholar] |
| 20. | Norte GE, Solaas H, Saliba SA, Goetschius J, Slater LV, Hart JM. The relationships between kinesiophobia and clinical outcomes after ACL reconstruction differ by self-reported physical activity engagement. Phys Ther Sport 2019;40:1-9. [Google Scholar] |
Fulltext Views
4,712
PDF downloads
766




