Translate this page into:
Flatfoot among school-age children in Almadinah Almunawwarah: Prevalence and risk factors
2 Department of Orthopedic Surgery, College of Medicine, Taibah University, Almadinah Almunawwarah, Saudi Arabia
Corresponding Author:
Abdullah M Alsuhaymi
Taibah University, Almadinah Almunawwarah
Saudi Arabia
abdulla.194@hotmail.com
| How to cite this article: Alsuhaymi AM, Almohammadi FF, Alharbi OA, Alawfi AH, Olfat MM, Alhazmi OA, Khoshhal KI. Flatfoot among school-age children in Almadinah Almunawwarah: Prevalence and risk factors. J Musculoskelet Surg Res 2019;3:204-208 |
Abstract
Objectives: Children with flatfoot are more vulnerable to have foot pain, foot injury, stress fractures, knee pain, and poor exercise performance. Some children may not experience any of these symptoms and the only predominant complaint would be foot pain. Flatfoot is considered a health issue that was not studied well in Saudi Arabia. The study aims to determine flatfoot prevalence among school-age children 7–14 years in Almadinah Almunawwarah and to know the effect of age, gender, and body mass index on the prevalence of flatfoot. Furthermore, a secondary aim is to find if there is a relationship between flatfoot and postactivity foot pain and participation in sports.Methods: This is a cross-sectional analytic study conducted on children aged 7–14 years living in Almadinah Almunawwarah, Saudi Arabia. Flatfoot was diagnosed using Staheli's Plantar Index. Binary logistics regression was used to predict the likelihood effect of sociodemographic data among children with flatfoot.
Results: A total of 403 children had been voluntarily recruited in this study. Boys were 193 (47.9%) while 210 (52.1%) were girls. The prevalence of flatfoot was 29.5% (119), 96.6% of them were flexible flatfeet and a relatively very low incidence (3.4%) of rigid flatfeet. Age has a significant relationship on the prevalence of flatfoot (P = 0.050) where 7–8-year-old group was rated highest among other age groups in the prevalence of flatfoot.
Conclusion: We found 29.5% of the children had flatfoot in the study sample. This prevalence is still high in comparison to developed countries. Furthermore, this study found a significant association between age and flatfoot in children.
Introduction
Flatfoot (pes planus) is a common condition.[1] It is diagnosed when the foot has a low or no longitudinal arch during weight-bearing. Around 90% of all clinical visits related to feet problems in children are due to flatfeet. It rarely causes disability but still stays one of the main concerns for the parents and grandparents.[2] In fact, it is a problem consisting of a group of physical features that include extreme eversion of the subtalar complex during weight-bearing, with plantar flexion of the calcaneum in relation to the tibia, plantar flexion of the talus, abduction and dorsiflexion of the navicular, abduction of the forefoot, and valgus posture of the heel.[3],[4]
There are two major types of flatfeet as follows: flexible flatfeet (FFF) and rigid flatfeet. FFF begins in childhood and continued into adulthood and usually affects both feet. It is the most common type. The term flexible defined as a medial longitudinal arch of the foot that collapses in various degrees when standing and returns to normal if the foot is not weight-bearing.[5]
There are many causes of flatfeet, causes of FFF include accessory navicular bone, generalized ligamentous laxity, neurologic disorders (cerebral palsy and hypotonia), muscular abnormalities (muscular dystrophy), genetic syndromes (osteogenesis imperfecta, Down syndrome, and Marfan's syndrome), collagen disorders such as Ehlers–Danlos, and other biomechanical causes such as ankle equines and valgus deformities. On the other hand, most rigid flatfeet are related to underlying pathology, including trauma, iatrogenic, tarsal coalition, congenital vertical talus, and peroneal spastic flatfoot.[6],[7],[8]
Children with flatfoot are more vulnerable to have foot pain, foot injury, stress fractures, knee pain, and poor exercise performance. Some children may not experience any of these symptoms, and the only predominant complaint is foot shape or the fact that they get fatigued easily.[9]
There are four methods that can be used to diagnose flatfoot, including (a) visual inspection,[10] (b) anthropometric values,[11],[12] (c) footprint parameters,[13] and (d) radiographic techniques.[14],[15] Many studies have been conducted worldwide about the prevalence of flatfeet in children. Many of these studies have determined the relationship between the prevalence of the flatfeet and the body mass index (BMI), age, and gender. Pourghasem et al.[16] found that obesity is one of the significant factors that cause an increase in the prevalence of flatfeet. A Nigerian study found that about one in every five children (6–10 years old) would be diagnosed with flat foot anomaly, and obesity further increased the risk.[17] Vergara-Amador et al. performed a study in Colombia and found a relationship between flatfoot with age, gender, and BMI. However, male gender and obesity were considered as risk factors.[18] Another study was in Taiwan also approved the relationship between flatfoot prevalence and obesity.[19] A study performed in China on children 6–13 years old exhibited that occurrence of FFF is directly proportional to BMI and the height, but it decreases with age.[20] A study done in Pakistan showed that flat foot was more common in males.[21] The previous studies showed a positive correlation between increased BMI, male gender, and flatfoot. In addition, they stated that flatfeet prevalence decreased with age.[16],[17],[18],[19] There was another study done in Iran that showed there was no gender difference in the flatfoot prevalence.[22]
Flatfoot is a health issue that was not studied well in Saudi Arabia at school-age children.
This study aims to determine flatfoot prevalence among school-age children (7–14 years old) in Almadinah Almunawwarah and to know the effect of age, gender, and BMI on the prevalence of flatfoot. Furthermore, to find if there is any relationship between flatfoot and postactivity foot pain and participation in sports.
Materials and Methods
A cross-sectional analytic study was conducted in various summer schools distributed within Almadinah Almunawwarah, Saudi Arabia, on children (7–14 years old) from May to July 2018.
The sample size was calculated and found to be 384. After obtaining informed consent from parents or legal guardians and explaining the objectives of the study, an interview with each child was started using a structured data collection sheet, which was directed by the investigators. The data collected included age, gender, participation in sports, history of pain in the foot and ankle after physical activity, weight, and height (BMI was calculated).
The participants were told and reassured that their participation in the study was voluntary and confidential. The study was anonymous; all information remained confidential. Confidentiality and privacy were maintained by data coding to eliminate identifying data with personal information.
The age was rounded off to the closest number, using 12 months as a unit. The ones from 8 years and 7 months to 9 years and 6 months were grouped into age 9 group and the ones from 9 years and 7 months to 10 years and 6 months were grouped into age 10 group. The footprint method was used on both feet (Foot imprinter Apex Harris Mat Set) and calculated Staheli's Arch Index[23],[24] to diagnose flatfoot. For the footprint [Figure - 1], we drew a tangential line to medial side of the metatarsal and heel region then, from midpoint of this line, we drew a perpendicular line to cross the footprint (we measured the width that was covered with ink from the medial side to the lateral side of the midfoot and called it A value). We drew another perpendicular line at the heel region from the tangential line across the footprint (we measured the width that was covered with ink from the medial side to the lateral side of the rear foot and called it B value). Staheli's Arch Index was calculated by dividing the value of A by the value of B, a child was considered having flatfoot if he/she had a Staheli's Plantar Arch Index >1.15.[24]
![[Figure - 1]](#fig_SaudiOrthopJ_2019_3_2_204_252281_f1.jpg){kind=link}
 |
| Figure 1: Staheli's Plantar Arch Index measures the width of the foot in the area of the arch and heel and the index is the ratio between these measurements |
A tiptoe standing test was done for each child with flatfoot from the footprint test to differentiate between FFF and rigid flatfeet. If the arch appeared and heels were turned into varus, then it was considered a FFF, if not, it was considered a rigid foot.
Our inclusion criteria were age between 7 and 14 years and living in Almadinah Almunawwarah city. Exclusion criteria were neuromuscular patients, congenital anomalies in the lower limb, and history of surgery, fracture, and dislocation in legs or feet. Furthermore, young children who could not answer the pain questions and were not accompanied by their mothers were excluded from the study.
The statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 22.0 (IBM, Armonk, New York, USA). The Chi-Square analysis was applied to compare the differences between the groups included in the study, and P < 0.05 was considered statistically significant.
Results
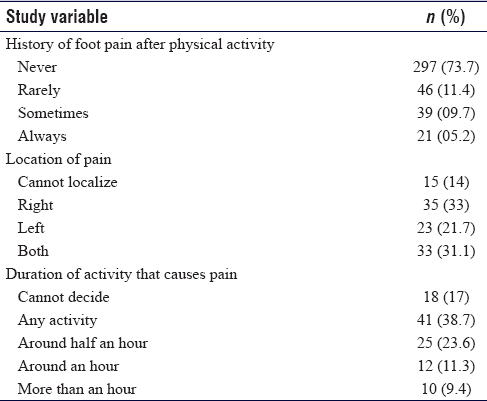
A total of 403 children had been voluntarily recruited in this study. Participants were divided into four age groups. The sample was almost evenly distributed between the four age groups. Age range was from 7 to 14 years old; Group A (7–8 years old) were 102 (25.3%), Group B (9–10 years old) were 106 (26.3%), Group C (11–12 years old) were 102 (25.3%), and Group D (13–14 years old) were 93 (23.1%). Boys were 193 (47.9%) while 210 (52.1%) were girls. Majority (65%) of the children were underweight (less than the 5th percentile), 26.1% were normal weight (5th percentile to less than the 85th percentile), 5.7% were overweight (85th to less than the 95th percentile), and 3.2% were obese (equal to or greater than the 95th percentile according to Centers for Disease Prevention and Control.[25] Around one-third (32.5%) of the children rarely participated in the sports, and 10.4% of the children never participated in the sports [Table - 1]. The majority of the study sample (73.7%) never had foot pain after physical activity, and 5.2% were having foot pain after physical activity [Table - 1]. Among the total number of children with foot pain, 33% had right foot pain, 21.7% had left foot pain, and 31.1% had pain on both feet. Pain started after a short duration of sports activity in 38.7% of the participants, whereas the others had it after more activity [Table - 1].
![[Table - 1]](#tbl_SaudiOrthopJ_2019_3_2_204_252281_t2.jpg){kind=link}
[Table - 2] shows the prevalence of flatfeet among the study participants.
![[Table - 2]](#tbl_SaudiOrthopJ_2019_3_2_204_252281_t3.jpg){kind=link}

Age was found to have a significant relationship to flatfoot (P = 0.050) where 7–8 years group was rated highest among other age groups in the flatfoot category while 13–14 was more in the normal foot category. Gender, classification according to BMI, participation in sports, and history of foot pain after physical activity showed no significant relationship to flatfoot [Table - 3].
![[Table - 3]](#tbl_SaudiOrthopJ_2019_3_2_204_252281_t4.jpg){kind=link}

A logistics regression analysis has been performed and is shown in [Table - 4], to ascertain the likelihood effect of sociodemographic characteristics among the children with flatfoot. Analysis revealed that age in years such as 9–10 age group (odds ratio 0.410, P = 0.009), 11–12 age group (odds ratio, P = 0.039), and 13–14 age group (odds ratio 0.468, P = 0.026) were all having a significant effect on the prevalence of flatfooted group of children.
![[Table - 4]](#tbl_SaudiOrthopJ_2019_3_2_204_252281_t5.jpg){kind=link}

Discussion
The prevalence of flatfoot in this study was 29.5% (119/403). Several published studies in the same context showed similar findings.[17],[18],[22] A study from Pakistan reported the lowest prevalence with 14.8%.[21] A study from Iran reported the highest prevalence among primary school students with 74%.[26] This prevalence is far too high compared to our study findings and the other published papers.
In this study, we found that 96.6% out of 119 children with flatfoot were FFF and a relatively low incidence (4; 3.4%) of rigid flatfeet. Among total children with flatfoot, 46.2% were unilateral and 53.8% were bilateral. Our result showed that rigid flatfeet was close enough to the study published in Iran where they reported an incidence of 6.1% of rigid flatfeet.[22] In Nigeria, they reported that among 106 participants with flatfoot, 12.3% were rigid flatfeet, with 8.5% unilateral, and 91.5% bilateral.[17] Our study results had shown identical findings of the type of flatfoot. This outline can be further validated from the study published in Pakistan where they found the incidence of rigid flatfeet to be 10% of participants while bilateral flatfeet were seen in 76.4%.[21]
When measuring the relationship between sociodemographic data to the groups of children with flatfoot it shows; age has a significant relationship with flatfeet while gender, classification according to BMI, participation in sports, and history of foot pain after physical activity showed no significant relationship to flatfoot. Binary logistics regression analysis revealed that age has a significant effect on the children with flatfoot. Few of the published articles indicated the association between sociodemographic characteristics and participants with flatfoot.[17],[22] On the contrary, Askary Kachoosangy and Aliabadi failed to prove the association between age and gender among primary school students with flatfoot.[26] While Vergara-Amador et al. found that age, city, gender, and BMI were likely to have a significant effect on children with flatfoot.[18] In general, although each study has their own description of children with flatfoot, still the finding of our study is substantial enough to supplement the findings of those researchers examining the phenomena of this study discipline.
Limitations
We faced some limitations while conducting this study such as there was inconsistency in evaluation methods and definitions of flatfoot used by other studies, also the foot pain was very subjective, which was based on children description. Finally, lack of prior studies to compare with on the same topic and same age group in our region.
Conclusion
We found 29.5% of the children in our sample from Almadinah Almunawwarah had flatfoot. This prevalence is still high in comparison to those of developed countries. Furthermore, this study found a significant negative association between age and flatfoot.
Ethics approval
The study received ethical approval from the Research Ethics Committee at the College of Medicine, Taibah University, Almadinah Almunawwarah Saudi Arabia, and the ID is 055-1439).
Acknowledgement
The authors gratefully acknowledge the help of the following medical students as data collectors: Rahaf Mohammed Alharbi, Nosaiba Saleh Alharbi, Sarah Abdulmohsen Almuzaini. We also, would like to thank everyone who participated in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Author's contributions
AMA, FFA, OAA, AHA, MMO, OAA and KIK conceived and designed the study, conducted research, provided research materials, and collected and organized data. All the authors analyzed and interpreted data. All authors wrote initial and final draft of the article and provided logistic support. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
| 1. | Evans AM, Rome K, Peet L. The foot posture index, ankle lunge test, beighton scale and the lower limb assessment score in healthy children: A reliability study. J Foot Ankle Res 2012;5:1. [Google Scholar] |
| 2. | Pfeiffer M, Kotz R, Ledl T, Hauser G, Sluga M. Prevalence of flat foot in preschool-aged children. Pediatrics 2006;118:634-9. [Google Scholar] |
| 3. | Canale ST. Pes planus. Campbells Operative Orthopaedics. 10th ed. St. Louis: Mosby; 2012. p. 4017-42. [Google Scholar] |
| 4. | Cappello T, Song KM. Determining treatment of flatfeet in children. Curr Opin Pediatr 1998;10:77-81. [Google Scholar] |
| 5. | Flexible Flatfoot – Foot Health Facts. University of Maryland Medical Center; 2018. Available from: https://www.umms.org/ummc/healthservices/orthopedics/services/pediatric/flat-feet. [Last updated on 2018 Mar 30; Last accessed on 2018 Dec 13]. [Google Scholar] |
| 6. | Flatfeet/Vertical Talus/Tarsal Coalition; 2018. Available from: https://www.umms.org/ummc/health-services/orthopedics/services/pediatric/flat-feet. [Last accessed on 2018 Mar 28]. [Google Scholar] |
| 7. | Mosca VS. Flexible flatfoot in children and adolescents. J Child Orthop 2010;4:107-21. [Google Scholar] |
| 8. | agerman SE, Cross MB, Positano R, Doyle SM. Evaluation and treatment of symptomatic pes planus. Curr Opin Pediatr 2011;23:60-7. [Google Scholar] |
| 9. | Omey ML, Micheli LJ. Foot and ankle problems in the young athlete. Med Sci Sports Exerc 1999;31:S470-86. [Google Scholar] |
| 10. | Evans AM, Nicholson H, Zakarias N. The paediatric flat foot proforma (p-FFP): Improved and abridged following a reproducibility study. J Foot Ankle Res 2009;2:25. [Google Scholar] |
| 11. | Evans AM, Rome K. A cochrane review of the evidence for non-surgical interventions for flexible pediatric flat feet. Eur J Phys Rehabil Med 2011;47:69-89. [Google Scholar] |
| 12. | Razeghi M, Batt ME. Foot type classification: A critical review of current methods. Gait Posture 2002;15:282-91. [Google Scholar] |
| 13. | Chen KC, Yeh CJ, Kuo JF, Hsieh CL, Yang SF, Wang CH, et al. Footprint analysis of flatfoot in preschool-aged children. Eur J Pediatr 2011;170:611-7. [Google Scholar] |
| 14. | Kanatli U, Yetkin H, Cila E. Footprint and radiographic analysis of the feet. J Pediatr Orthop 2001;21:225-8. [Google Scholar] |
| 15. | Harris EJ, Vanore JV, Thomas JL, Kravitz SR, Mendelson SA, Mendicino RW, et al. Diagnosis and treatment of pediatric flatfoot. J Foot Ankle Surg 2004;43:341-73. [Google Scholar] |
| 16. | Pourghasem M, Kamali N, Farsi M, Soltanpour N. Prevalence of flatfoot among school students and its relationship with BMI. Acta Orthop Traumatol Turc 2016;50:554-7. [Google Scholar] |
| 17. | Ezema C, Abaraogu U, Okafor G. Flat foot and associated factors among primary school children: A cross-sectional study. Hong Kong Physiother J 2014;32:13-20. [Google Scholar] |
| 18. | Vergara-Amador E, Serrano Sánchez RF, Correa Posada JR, Molano AC, Guevara OA. Prevalence of flatfoot in school between 3 and 10 years. Study of two different populations geographically and socially. Colomb Med (Cali) 2012;43:141-6. [Google Scholar] |
| 19. | Chen JP, Chung MJ, Wang MJ. Flatfoot prevalence and foot dimensions of 5- to 13-year-old children in Taiwan. Foot Ankle Int 2009;30:326-32. [Google Scholar] |
| 20. | Yin J, Zhao H, Zhuang G, Liang X, Hu X, Zhu Y, et al. Flexible flatfoot of 6-13-year-old children: A cross-sectional study. J Orthop Sci 2018;23:552-6. [Google Scholar] |
| 21. | Ali M, Asad Ullah M, Amjad I. Prevalence of the flat foot in 6-10 years old school going children. Rawal Med J 2013;38:385-7. [Google Scholar] |
| 22. | Sadeghi-Demneh E, Jafarian F, Melvin JM, Azadinia F, Shamsi F, Jafarpishe M, et al. Flatfoot in school-age children: Prevalence and associated factors. Foot Ankle Spec 2015;8:186-93. [Google Scholar] |
| 23. | Engel GM, Staheli LT. The natural history of torsion and other factors influencing gait in childhood. A study of the angle of gait, tibial torsion, knee angle, hip rotation, and development of the arch in normal children. Clin Orthop Relat Res 1974;99:12-7. [Google Scholar] |
| 24. | Hernandez AJ, Kimura LK, Laraya MH, Favaro E. Calculation of Staheli's plantar arch index and prevalence of flat feet: A study with 100 children aged 5-9 years. Acta Ortop Bras 2007;15:68-71. [Google Scholar] |
| 25. | Healthy Weight. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention; 2018. Available from: https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html. [Last accessed on 2018 Dec 12]. [Google Scholar] |
| 26. | Askary Kachoosangy R, Aliabadi F. Prevalence of flat foot: Comparison between male and female primary school students. Iran Rehabil J 2013;11:22-4. [Google Scholar] |
Fulltext Views
2,860
PDF downloads
1,397




