Translate this page into:
Gulf cooperation council female residents in orthopedics: Influences, barriers, and mental pressures: A cross-sectional study
2 Department of Orthopedics, Oman Medical Specialty Board, Muscat, Oman
3 Department of Orthopedics, King Faisal Specialist Hospital & Research Center, Musculoskeletal Surgical Oncology Fellowship Training Program, Riyadh, Saudi Arabia
4 Department of Orthopedics, AlRazi Hospital, Kuwait Institution for Medical Specializations, Kuwait City, Kuwait
5 College of Medicine, Taibah University, Almadinah Almunawwarah, Saudi Arabia
6 Department of Orthopedics, College of Medicine, Taibah University, Almadinah Almunawwarah, Saudi Arabia
Corresponding Author:
Abdulmuhsen N Alshammari
Pediatric Orthopedic Surgery Fellow, King Faisal Specialist Hospital and Research Center, Riyadh
Saudi Arabia
m_shamari@hotmail.com
| How to cite this article: Alshammari AN, Shafiq MO, Altayeb MA, Khaja AF, Ghabban KM, Khoshhal KI. Gulf cooperation council female residents in orthopedics: Influences, barriers, and mental pressures: A cross-sectional study. J Musculoskelet Surg Res 2018;2:51-56 |
Abstract
Objectives: There is insufficient data about female orthopedic residents in the Gulf Cooperation Council (GCC) region. This study was performed to survey what influences females to take up orthopedics, and the barriers, mental pressures, and obstacles they face while a resident in training. Methods: This is a cross-sectional study, which was conducted using an online self-reported validated questionnaire. Our population consisted of 569 orthopedic trainees who met our inclusion criteria, and we received 254 anonymous responses (44.6%). Results: The response rate was 78.7% for females (37 out of 47 total females who were sent the questionnaire) and 41.6% for males (217 out of 522 total number of males). The gender distribution of those who responded was 14.6% (n=37) females and 85.4% (n=217) of males. Around half of the females (48.6%) in the study decided to join orthopedic programs during their undergraduate studies. The majority of female residents (75.7%) agreed that orthopedics is physically tiring and 89.2% of them agreed that there are gender intolerances. The need to increase the number of female residents was another notion shared by 86.5% of them. On the contrary, 62.2% of the male responders disagreed to the need of increasing the female orthopedic residents and 34% were with the opinion that female residents are not fit to cover on-call duties. Conclusion: Gender intolerances exist in the GCC orthopedic programs. This might discourage female physicians from pursuing orthopedic careers. All of the concerns raised by the residents are adjustable and attainable, such as offering maternity leaves, encouraging positive behavioral changes in male surgeons, and providing equal opportunities for applicants to orthopedic boards' acceptance.Introduction
Since the establishment of the Gulf Cooperation Council (GCC) in 1981, there have been agreements and achievements in multiple aspects including health systems. An exact estimate of the number of doctors working in this region remains tricky to establish, with the latest available report (2009) showing that there were 80,635 doctors.[1] This number is believed to have dramatically increased since then. In the recent times, observing the medical field in the region, there is no apparent gender discrimination but the idea of gender imbalance is strongly present among health professions and there is a belief that gender discrimination in surgical specialties in specific may be present, as reported by Hannawi and Al Salmi and Baqi et al.[2],[3]
Previous studies, including Miller and LaPorte, have shown that orthopedics as a career has a lot of occupational hazards (radiation) and risks to pregnancy, which perhaps is one of the concerns that might be preventing females from taking orthopedics as a specialty.[4],[5],[6] Another reason might be the lack of a well-described policy for maternity and paternity leaves, though that is common to all other specialties.[5] Could the absence of senior female orthopedic surgeons as role models and the lack of clinical exposure in early years be reasons for females not choosing the branch?[6],[7] There is also no established society for female orthopedic surgeons in our region, similar to the Ruth Jackson Orthopaedic Society in the USA.[7]
Reasons are unclear for gender intolerances if they exist among orthopedic surgeons or about the barriers and mental pressures that females face in orthopedics, and there is no enough literature to support the presence of gender intolerance. Taking into consideration all the barriers, some of the female orthopedic surgeons are planning to reduce the working hours after residency or to work as part-timers in their future plan, as described by Hariri et al.[8] An obstacle we have faced during the preparation of this manuscript is the lack of sufficient data about female orthopedic surgeons in the region.
We believe that there is a large demand and need for orthopedic surgeons in general and for gender diversity in the region. In Middle Eastern culture, many female patients prefer to be seen by female physicians and a good number of them might refuse to be examined by a male physician if it involves exposure of intimate areas.
The primary objective of this study is to gain insight from female orthopedic residents and recent graduates of the accredited training programs in the GCC about what influenced them to join orthopedics, the nature and kind of barriers they faced, and the mental pressures experienced within the residency and thereafter. A secondary objective was to look at the male perspective and their opinion regarding the presence of gender intolerance, how they looked at the issue of barriers and mental pressures, and the need to increase the number of female residents. We believe this to be the first research article holding this interest.
Materials and Methods
This is a cross-sectional study, based on a questionnaire designed electronically and distributed individually using a web link starting October 2017. The targeted population in this survey was residents who are registered as orthopedic trainees in the accredited programs at the selected countries at the time of distribution, as well as those who had graduated and completed their training from 2013 to 2016 as the majority of females have joined the training during this period. We excluded individuals who were not registered as orthopedic residents and those who completed the training before 2013 to eliminate and reduce recall bias. We also excluded those who newly joined the training programs postgraduate year 1 due to lack of experience, which could potentially affect the reliability of the results. Our population consisted of 569 orthopedic trainees (both males and females) who met our study criteria. We received 254 anonymous responses, all of which met the inclusion criteria and were included in the study.
The survey addressed three broad categories. The first category was about general and personal information including gender, marital status and number of children if any, the country of the residency program, level of training, and year of graduation. The second category was about the reason of choosing orthopedics; individuals were asked to choose from the provided reasons for joining the specialty, with a separate box to specify other reasons that were not mentioned. The last category was about gender intolerances and differences in the specialty divided into two sections. There was a common section, which had to be answered by both male and female residents and one section each, which was gender specific with close-ended questions (yes/no answers). Estimated time for completing the survey was 6–8 min, which consisted of 33 items. Along with two orthopedic residency program directors, three independent biostatisticians, an academic educator, a chief resident, and a psychiatrist, we reviewed the questionnaire for biases, ease of language, and clarity. A pilot study was preformed, feedback was collected, and changes were made before a final questionnaire was distributed.
The ethical approval was obtained from the Research Ethical Board Committee, Taibah University, Almadinah Almunawwarah, Saudi Arabia. Each individual consented for participation at the beginning of the survey and was informed that participation is voluntary and given the option to decline. All participants agreed to participate and none declined the survey. Our questionnaire was designed using Google Forms. The data collected were then transferred into a comma-separated value extension file, which was used and analyzed using the Statistical Package for the Social Sciences program, version 22.0 (Armonk, New York, USA) for descriptive statistics.
Results
Out of the target population (569), we received 254 anonymous responses, giving us a response rate of 44.6%. Female responders accounted for 14.6% (n = 37) and they represented 78.7% from the total female population who satisfied the inclusion criteria (n = 47). [Table - 1] shows the biographical data including a breakdown of responders across gender, response rate, level of residency training, etc.
![[Table - 1]](#tbl_SaudiOrthopJ_2018_2_2_51_230794_t4.jpg){kind=link}
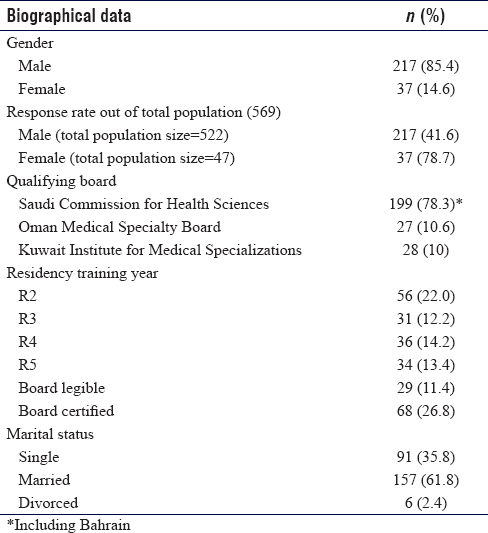
As for the influences, 48.6% of female participants decided to enter orthopedics during their undergraduate studies, 24.3% of them chose it during an internship rotation in orthopedics, and 16.2% of them chose it after the internship. Based on their personal interest, 78.4% chose orthopedics and 37.8% chose it because of the challenge that orthopedics provides. Female residents were less likely to choose orthopedic surgery for financial reasons, prestige, and parental pressure as percentages of these factors were quite low at 5.4%, 5.4%, and 2.7%, respectively.
A total of 78.4% of the female residents were single, only 16.2% were married (8.1% had one child and 8.1% had two children), and 5.4% were divorced [Figure - 1]. In contrast, 69.6% of male residents were married and 56.2% had children.
![[Figure - 1]](#fig_SaudiOrthopJ_2018_2_2_51_230794_f1.jpg){kind=link}
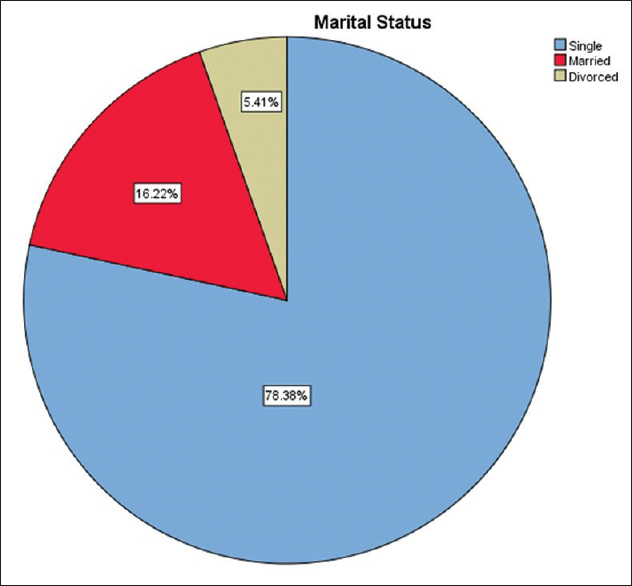 |
| Figure 1: Marital status of female residents in the study |
Almost two-thirds of the female residents (62.2%) stated that they find matching into orthopedic residency as rather difficult, as opposed to male residents.
In regard to the pressures female residents face, they were predominantly physical exhaustion and gender intolerance. About 75.7% of the female residents agreed that orthopedics is physically tiring and, surprisingly the percentage, though it looked high, was less than their male counterpart, which was 89.4%. Two-thirds of both female and male residents felt burned out and exhausted equally (67.6% and 67.7%, respectively). The residents who shared the opinion that orthopedics had negatively impacted their lives were 33.6% males and 13.5% females.
Female residents who agreed that gender intolerances in orthopedics exist were 89.2%. Male residents (61.8%) had the opinion that female residents are not of equal caliber regarding handling physical activities and workload. The majority of male residents (65.9%) agree that female residents are fit to cover on-call duty and 62.2% state that the number of female orthopedic residents does not need to be increased. Interestingly enough when asked if there are gender intolerances in their programs against females, about 60% of them agreed that there are.
However, in contrast to the information above, 86.5% of the female residents agreed that the number of female orthopedic residents needs to be increased, with 94.6% going on to say that this will help the community at large. Quiet a high number of females (73%) agreed that if they get maternity support, the interest rate of females applying to orthopedics would increase.
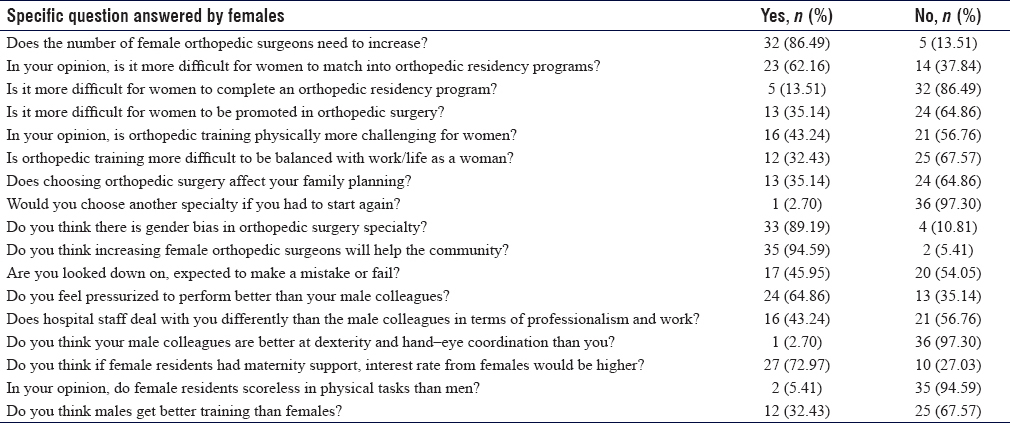
For the female-only part of the questionnaire, 67.6% of female residents answered that they do not think being an orthopedic resident is difficult with work or life balance [Table - 2]. Regarding family planning, 64.9% agreed that their family planning was not disturbed by orthopedics.
![[Table - 2]](#tbl_SaudiOrthopJ_2018_2_2_51_230794_t5.jpg){kind=link}
If offered to retake another program or change their choice, 97.3% of the female residents did not wish to do so. [Figure - 2] shows that 21.6% of the female residents are undecided about their future fellowship plans but are interested in shoulder and upper limb surgery and then pediatric orthopedics at 18.9% and 16.2%, respectively. Male residents are more likely to choose sports medicine and arthroplasty (17.5% each). While 10.8% of the female residents expressed interest in sports medicine, none of the female residents were interested in the field of arthroplasty.
![[Figure - 2]](#fig_SaudiOrthopJ_2018_2_2_51_230794_f2.jpg){kind=link}
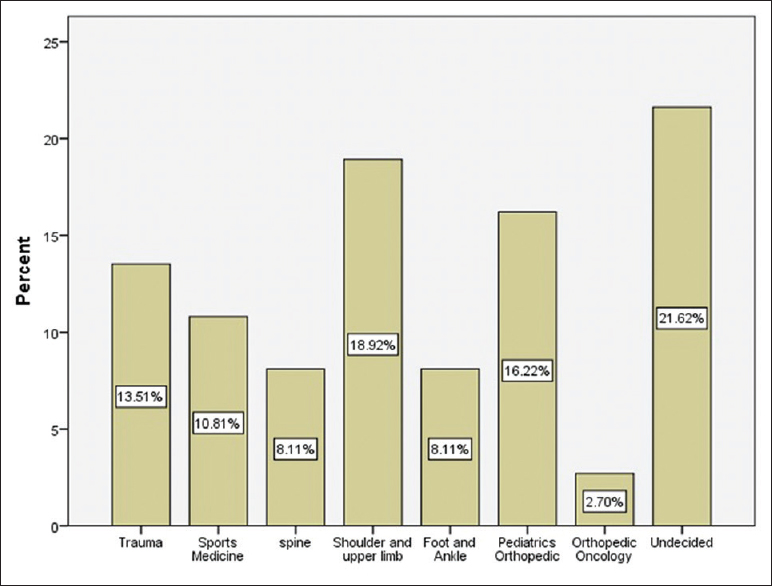 |
| Figure 2: Female residents' interest in subspecialties |
Discussion
The survey further acknowledged that 62.0% of the female participants found acceptance into orthopedic programs difficult. Since there are not many females in orthopedics in the GCC, it is perhaps viewed by program directors as a risk, to invest in a female candidate, while some may still think of orthopedics as a male-only specialty. Some of the regularly asked questions in females' interviews include: “are you married?” “do you have children?” and “what will you do if you become pregnant?”[9] Even if the female candidate is outstanding, there is always some reservation from program directors that she might not be able to complete her residency. This notion might stem from the programs facing a few cases of female residents leaving the program for social or personal reasons, forgetting that even males at times leave their residency for social or personal reasons. However, about 86.0% of the female participants do not think it is more difficult to complete an orthopedic residency and 64.9% feel that they are pressurized to perform better than their male peers to overcome the perceived male–female difference.
About 45.9% of the female residents feel that they are looked down upon and expected to fail. Around 35.0% of them think that it is more difficult for a female to get promoted in orthopedics. About 43.2% have experienced different treatment by hospital staff in terms of unprofessional conduct, whether they are looked down upon, they get less operating time, or receive remarks that they should consider a career change.
Despite the buildup of all these factors seemingly at their disadvantage, they deliver, at least just as well as their male peers.[10] When it came to thoughts on who received better training, 33.6% of the males thought females got better training, whereas 32.4% of the females thought the case to be the other way around. From this, it seems that training opportunities are equal to both males and females, as there is no quantifiable evidence that training chances differ and no official complaints have been put forward.
A large number of surgeries require intraoperative imaging; this, in turn, serves as another burden these females might face during and after they complete their training. One would think that intraoperative imaging and radiation hazard protocols ensure all the staff's safety, but realistically, there are a lot of violations occurring for the pure intention of time-efficient practice. In our study, 73.0% of the female residents think that maternity leave would attract more females to apply to orthopedics and 64.9% of them do not think that it would affect their family planning. In addition, a confident and reassuring 67.6% reported that they had no trouble with their work–life balance. Among the factors that were investigated as potential dissuades for females applying to orthopedics were family planning and the ability to apply for maternity leave. Currently, all the addressed institutions in this study do not allow maternity leave. This confines female orthopedic surgeons in the GCC to only two potential routes for family planning, either starting a family before residency or after completion of training.
Our questionnaire asked a question to both genders, inquiring if they thought that there are gender intolerances in orthopedics. More than half of the males (59.9%) as well as the majority (89.2%) of the female residents agreed with this statement. As 87.6% of the males attributed this to orthopedics being more challenging for females, 56.8% of the females disagreed with the latter statement. Most of the female residents (94.6%) answered that they did not think they scored less in physical activity; by contrast, 69% of the male residents disagreed, even 34% of them went on to report that they deemed female residents unfit to cover on-call duties. When it came to questions about surgical skills, manual dexterity, and hand–eye coordination, 50% of the male residents answered that their skills were superior to their female colleagues. About 38.0% of them also answered that they do not think females can handle surgical orthopedic instruments. Again, it is believed by the authors that this is based on opinions without evidence, which is in keeping with gender intolerance. On the other hand, 97.3% of the female participants do not see a difference in their skill level compared with males. It could well be that they developed their tricks to compensate for their physical deficits if they exist. It could also be hypothesized that perhaps the actual strength needed to perform the procedure is adequate for a female resident or if there does exist a difference, then technique and biomechanics of the procedure being performed could be altered to better suit a female resident.
For 54.4% of the male residents who reported that they do not think female orthopedic surgeons have any added value to this community and the 62.2% of them who did not think that the number of females should increase in these surgical specialties, the answer is that the GCC community still has a large proportion where the males in the society prefer their female relatives and companions to be treated by female physicians, and some of the male doctors also fall into this category.[11] They might be right in that as Wallis et al. noted that female patients may suffer from potentially inadequate examination if they have wounds around their intimate body parts, due to male physician sensitivity issues, ultimately disadvantaging them.[12] A potential explanation for the male residents rejecting female residents could be that they prefer a male-dominant workspace, due to the cultural limitations, or simply their inability to have normal social interactions with female colleagues as per our culture, and wish to avoid any awkward interactions. On the other hand, the vast majority (94.6%) of the female surveyors believe that the community needs more female orthopedic surgeons and 86.5% of them think that the number of female-accepted applicants should be increased.
Job satisfaction is rather difficult to measure; however, we figured the best way to gain a general reflection on this, which was to ask the participants when and how did they decide to join orthopedics and whether or not they would choose it again if they had the option to change. Our study showed that 10.8% of female participants decided for a career in orthopedics before entering university and 48.6% of them during their undergraduate studies. Another 24.3% chose this path during their internship and 16.2% of them after internship [Figure - 3], whereas the percentages of male participants were 6.0%, 46.5%, 35%, and 12.5%, respectively. The contrast above highlights perhaps that a higher percentage of males (35.0% vs. 24.3%) chose the specialty based on practical experience as an intern compared to females. About 78.4% of our female participants reported that they chose orthopedics because they had a personal interest, out of which 37.8% were attracted to the challenges it provides. Female residents are less likely to choose orthopedics for financial reasons (5.4%) or prestige (5.4%). To the 97.3% of female participants who would choose to pick orthopedics again, it seemed that they were satisfied with the discipline in spite of the reservations they had on the training program. Surprisingly, male participants were less satisfied as only 77.9% would pick orthopedics again if they had another chance to choose. This might be due to the fact that a lower percentage of males chose orthopedics out of personal interest (56.2%). We noticed that females are more toward early interest in orthopedics, earlier career planning, and more job satisfaction than males.
![[Figure - 3]](#fig_SaudiOrthopJ_2018_2_2_51_230794_f3.jpg){kind=link}
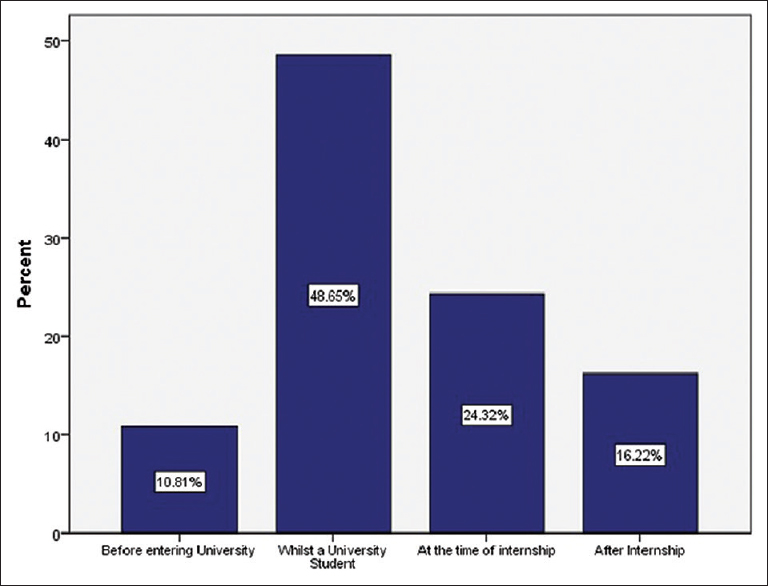 |
| Figure 3: Female residents responses based on a decision of joining orthopedic surgery |
It has been shown in this study that the 21.6% of the current GCC female orthopedic residents are still undecided about their choice of future fellowship. For instance, 18.9% are interested in shoulder and upper limb surgery, 16.2% reported interest in pediatric orthopedics, 10.8% expressed interest in sports medicine, and none of the female residents were interested in the field of arthroplasty [Figure - 2]. By observation, these are subspecialties, which deal with less radiological exposure and have a more predictable schedule than trauma surgery for example. However, it can also be said that these advantages are attractive to some of the male trainees as well.
Limitations
The response rate (78.7%) of female orthopedic residents in the Gulf region is one of the major strengths of this study, despite our relatively small sample size.
With this type of study, it was difficult to ascertain if the participants were truthful, as the data collection was in the form of a questionnaire and we did not have discussion groups with them directly. The study design limited us to more subjective and qualitative responses from our addressed population. The overall (males and females) response rate of 44.6% was achieved despite amplified efforts to distribute the questionnaire. This might be attributed to a lower interest in research by the orthopedics culture in our given area. This study is the first of its kind in the region, so we had no benchmark to use. Hence, this study might have been governed by a rather subjective approach susceptible to observer and analytical biases. We can only wish that this study provides an initial platform to influence more powerful reviews, improving our shortcomings.
Recommendations
We would suggest the need to investigate psychological implications directing people and doctors away from medicine as a whole and orthopedics specifically. The workforce in this area is in a great need for reinforcement, which should be encouraged by the postgraduate training systems in the GCC. Sociological studies in the area should be conducted to highlight the community needs to ensure avoiding misconduct and optimize health-care services.
It would also be beneficial to understand what guides orthopedic surgeons to choose specific subspecialties. This will enable training programs to estimate deficiencies in workforces and sustainability of specific subspecialty teams.
We also recommend allowing female orthopedic residents to take a year off from the program for family planning. During this year, they can choose to take an elective rotation in a medical field related to orthopedics, so they can avoid the heavy nature of orthopedic practice and radiation exposure altogether. Rotations in the field of pathology, radiology, rheumatology, plastic surgery or clinical anatomy are all elective options that can prove to be complementary to orthopedic practice. They can also spend a year doing a master degree in epidemiology, medical education, or clinical research methods. They may pursue a basic science research master degree or any complementary sciences that can improve orthopedic care; as a result, it would enhance the orthopedic care of patients and the family planning for the resident, leading to a win-win situation.
Finally, we encourage the conduction of further studies on the same topic using a qualitative type of research. We also recommend that they better include detailed trainers' perspectives as well.
Conclusion
Gender intolerances are experienced in the GCC orthopedic training, discouraging female physicians from pursuing surgical careers. Various barriers are encountered or are expected to be encountered by females during residency. All of the elements raised are adjustable, such as offering maternity leave, encouraging positive behavioral changes of male surgeons, and providing equal opportunities for applicants to orthopedic training. These females, however, are determined to push through and did not report any limitations for their future practice or subspecialty choices.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Authors contributions
All authors participated in conceiving and designing the study, reviewing the literature, and collecting and analyzing the data. ANA and MOS prepared the manuscript. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript. The authors testify that all persons designated as authors qualify for authorship and have checked the article for plagiarism.
| 1. | Secretariat General of the Gulf Cooperation Council. Gulf Information with Categorization; 2018. Available from: http://www.gcc-sg.org/enus/CognitiveSources/GulfDatabases/Pages/GulfInformationwithCategorization.aspx. [Last accessed on 2017 Oct 15]. [Google Scholar] |
| 2. | Hannawi S, Al Salmi I. Time to address gender inequalities against female physicians. Int J Health Plann Manage 2017;2:35. [Google Scholar] |
| 3. | Baqi S, Albalbeesi A, Iftikhar S, Baig-Ansari N, Alanazi M, Alanazi A, et al. Perceptions of gender equality, work environment, support and social issues for women doctors at a university hospital in Riyadh, Kingdom of Saudi Arabia. PLoS One 2017;12:e0186896. [Google Scholar] |
| 4. | Keene RR, Hillard-Sembell DC, Robinson BS, Novicoff WM, Saleh KJ. Occupational hazards to the pregnant orthopaedic surgeon. J Bone Joint Surg Am 2011;93:e1411-5. [Google Scholar] |
| 5. | Mayer KL, Ho HS, Goodnight JE Jr. Childbearing and child care in surgery. Arch Surg 2001;136:649-55. [Google Scholar] |
| 6. | Miller EK, LaPorte DM. Barriers to women entering the field of orthopedic surgery. Orthopedics 2015;38:530-3. [Google Scholar] |
| 7. | O'Connor MI. Medical school experiences shape women students' interest in orthopaedic surgery. Clin Orthop Relat Res 2016;474:1967-72. [Google Scholar] |
| 8. | Hariri S, York SC, O'Connor MI, Parsley BS, McCarthy JC. Career plans of current orthopaedic residents with a focus on sex-based and generational differences. J Bone Joint Surg Am 2011;93:e16. [Google Scholar] |
| 9. | Jefferson L, Bloor K, Maynard A. Women in medicine: Historical perspectives and recent trends. Br Med Bull 2015;114:5-15. [Google Scholar] |
| 10. | Pico K, Gioe TJ, Vanheest A, Tatman PJ. Do men outperform women during orthopaedic residency training? Clin Orthop Relat Res 2010;468:1804-8. [Google Scholar] |
| 11. | Shamrani H. A cross-sectional survey of women's provider gender preferences for gynecology and obstetrics care at King Abdulaziz University Hospital. J Womens Health Care 2016;5:347-54. [Google Scholar] |
| 12. | Wallis CJ, Ravi B, Coburn N, Nam RK, Detsky AS, Satkunasivam R, et al. Comparison of postoperative outcomes among patients treated by male and female surgeons: A population based matched cohort study. BMJ 2017;359:j4366. [Google Scholar] |
Fulltext Views
3,283
PDF downloads
1,212




