Translate this page into:
Humeral osteoid osteoma at deltoid tendon insertion: A case report and literature review
Corresponding Author:
Mohammed L Al-Otaibi
Department of Surgery, College of Medicine, King Khalid University, P. O. Box: 641, Abha
Kingdom of Saudi Arabia
mohammedlafiotaibi@gmail.com
| How to cite this article: Al-Otaibi ML. Humeral osteoid osteoma at deltoid tendon insertion: A case report and literature review. J Musculoskelet Surg Res 2017;1:16-18 |
Abstract
Osteoid osteoma predominates all symptomatic benign bone tumors in younger patients with an incidence reaching 10%. Night pain responding to nonsteroidal anti-inflammatory pain medication, especially aspirin is its pathognomonic symptom. Osteoid osteoma lesion in the bone at tendon insertion is difficult to diagnose with pain pattern becoming atypical; clinical signs and radiographic presentations are misleading and histological features altered. The osteoid osteoma at deltoid tubercle of the humerus is rare and missed in the initial presentation. This case report describes how an osteoid osteoma of the deltoid insertion of the humerus can be different.Introduction
Symptomatic benign bone tumors of osteoid osteoma predominate among younger patients with an incidence approaching 10% with night pain responding to nonsteroidal anti-inflammatory pain medication, especially aspirin described as the clinical presentation.[1],[2] Jaffe and Greenspan described the imaging differential diagnosis of this benign bone-forming lesions.[3],[4]
When an osteoid osteoma lesion appears in a bone at a tendon insertion it will be difficult to diagnose since the pain pattern may be atypical; clinical signs and radiographic presentations may be misleading and histological features of classic osteoid osteomas may be altered.[5] The osteoid osteoma at deltoid tubercle of the humerus is not common and often missed in the initial presentation.
It is not clear how trauma contribute to the development of osteoid osteoma although several authors reported posttraumatic presentation.[6],[7],[8],[9]
The typical night pain at the affected site of osteoid osteoma usually responds to aspirin and nonsteroidal anti-inflammatory medication, which block the inflammatory response of prostaglandins produced by the lesion.[10] The neural theory, which was postulated by other authors claiming that neural ends get excited by the high intraosseous tension due to the lesion increased hyperemia.[11],[12]
Direct stimulation of nerve endings by prostaglandins is another theory for the disease pathophysiology.[13] Nevertheless, painless lesions do exist.[14]
Here, the author reports a case of an osteoid osteoma in the deltoid insertion of left humerus and describing its symptoms, signs, radiographic appearance, intraoperative images, and the outcome after surgical removal of the lesion.
Case Report
A 26-year-old male patient presented with a history of pain about the nondominant shoulder. It was mainly nocturnal, precipitated by activity involving shoulder abduction, and relieved by aspirin. The patient denied any history of trauma or previous disease in the left shoulder. The condition had been diagnosed previously in another institute as impingement syndrome and was treated by two subacromial steroid injections and physical therapy, with no improvement of symptoms. In another occasion, direct steroid injection at the deltoid insertion was given with partial and transient improvement.
Physical examination of the left shoulder at presentation to our institute revealed no deformity or skin lesions. The range of active movements of the left shoulder was slightly limited by pain, though the passive motion was normal. Provocative abduction against resistance was very painful, and there was no evidence of rotator cuff involvement or shoulder instability.
There was a tender swelling of the proximal third of left arm and modest deltoid wasting, but no sensory disturbances. Laboratory profile was within normal reference range. The plain radiograph failed to show the typical nidus according to radiology report from the other institution.
Magnetic resonance imaging (MRI) of the left shoulder (done at the other institution) showed the typical osteoid osteoma at the deltoid tubercle that was surrounded by edema [Figure - 1]. Computerized tomography scan typically done in such cases was not done since MRI showed the typical diagnostic picture including the nidus. History, clinical and radiographic findings revealed to the diagnosis of an osteoid osteoma of the left humerus.
![[Figure - 1]](#fig_SaudiOrthopJ_2017_1_1_16_213067_f1.jpg){kind=link}
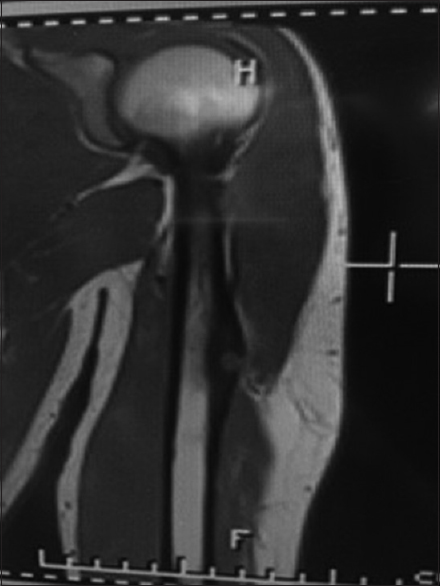 |
| Figure 1: Magnetic resonance image showing a typical nidus |
The patient was given the option to have this lesion treated with less invasive radiofrequency ablation, which is not available at our institution, yet he decides to undergo surgery to avoid traveling and delay. A direct lateral approach was used for the surgical excision. Intraoperative image intensifier was used to localize presumptive location [Figure - 2]. Total removal of the tubercle was not done to avoid deltoid weakness, rather deroofing was done using a small burr and the nidus was curetted with a small curette [Figure - 3]. A high-speed burr was used to remove the sclerotic bone inside the lesion and the defect was filled with bone wax. The arm was immobilized postoperatively for 2 weeks. Histological examination confirmed the diagnosis of osteoid osteoma. The pain disappeared immediately and completely after surgery. The patient was followed regularly in the outpatient clinic for 2 years. On the final visit, the patient symptoms disappeared completely and the radiographs were lesion free.
![[Figure - 2]](#fig_SaudiOrthopJ_2017_1_1_16_213067_f2.jpg){kind=link}
![[Figure - 3]](#fig_SaudiOrthopJ_2017_1_1_16_213067_f3.jpg){kind=link}
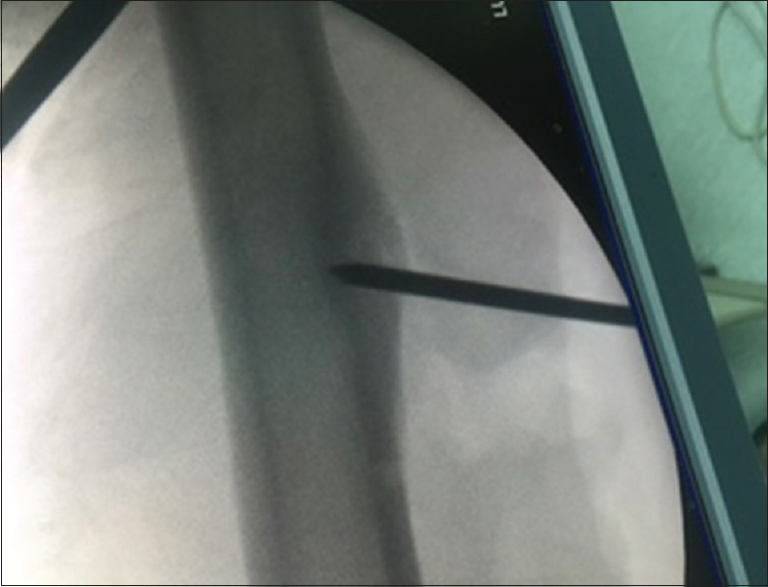 |
| Figure 2: Intraoperative image localizing of the lesion |
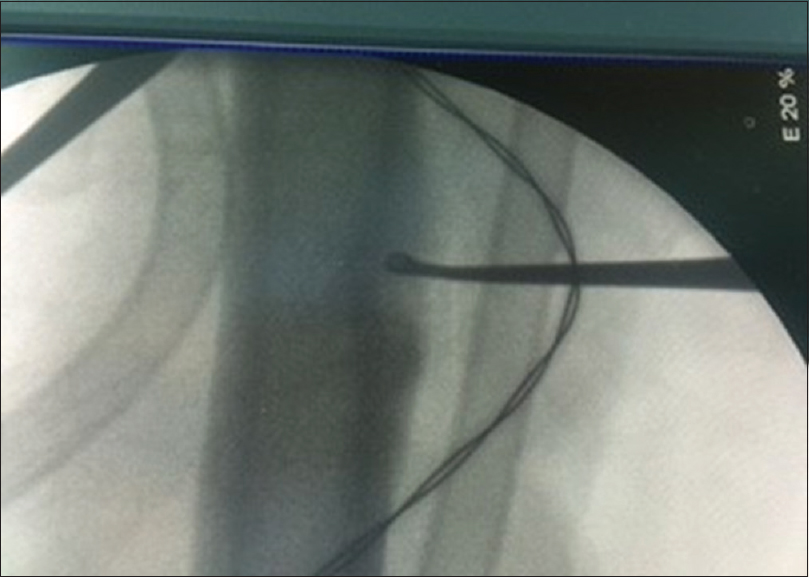 |
| Figure 3: Curettage of the lesion under image intensifier control |
Discussion
Reported cases of humeral osteoid osteoma are few while lesions affecting the metacarpal and the lower limb bones, especially the tibia predominates.[15] However, to the author's best knowledge the presence of osteoid osteoma at the deltoid tubercle was not reported before in the literature. Osteoid osteoma at this site needs special precaution during surgical treatment, mainly to perform deroofing using a high-speed burr then curating the nidus and to avoid en block excision, which could weaken the deltoid insertion.
Simple radiographs usually pick the typical nidus of the osteoid osteoma. Computed tomography may be required to localize a lesion that has not been seen on plain X-rays.[16],[17]
Symptomatic treatment usually initiated in managing such lesions, to cure the disease, while the nidus has to be surgically removed. Decoring or drill resection of the nidus,[18] followed by subsequent injection of ethanol [19],[20] and thermal destruction with laser photocoagulation [21] or radiofrequency ablation,[22] has been used for removal or destruction of the nidus.
Incomplete excision of nidus will lead to its recurrence,[23],[24] which was reported following decoring or drill resection and rarely after total removal with lesion free margins.
During the postoperative follow-up, successful eradication is assured with the disappearance of pain and swelling. Recurrences usually occurs 7 months after treatment,[25] they usually show nidus of 1.0–1.5 cm in diameter.[26]
In musculoskeletal conditions, symptoms often are modified according to the anatomic location of the pathology, and anatomical location of the pathology may dictate the management plan. This case report shows how that osteoid osteoma of the deltoid tubercle can be a diagnostic and management challenge.
Conclusion
Osteoid osteoma at deltoid tendon insertion, although rare, could be considered as one of the differential diagnoses of chronic pain about the shoulder of a young active patient regardless of trauma. Osteoid osteoma of the humerus at deltoid tendinous insertion is challenging as to its treatment, and particular precautions should be taken during its surgical excision.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Authors contributions
MLO conceived, designed the study, conducted research, searching research materials, and collected, organized data, analyzed and interpreted data. And finally MLO wrote initial and final draft of the article. The author critically reviewed and approved the final draft and is responsible for the content and similarity index of the manuscript.
| 1. | Heine J. Einheilender knochensequester und der grundphalanx des ringfingers. Arch Klin Chir 1927;146:737. [Google Scholar] |
| 2. | Bergstrand H. Über eine eigenartige, wahrscheinlich bisher nicht beschriebene osteoblastische Krankheit in den langen Knochen der Hand und des Fusses. Acta Radiol 1930;11:596. [Google Scholar] |
| 3. | Jaffe H. A benign osteoblastic tumor composed of osteoid and atypical bone. Arch Surg 1935;31:709. [Google Scholar] |
| 4. | Greenspan A. Benign bone-forming lesions: Osteoma, osteoid osteoma, and osteoblastoma. Clinical, imaging, pathologic, and differential considerations. Skeletal Radiol 1993;22:485-500. [Google Scholar] |
| 5. | Burger IM, McCarthy EF. Phalangeal osteoid osteomas in the hand: A diagnostic problem. Clin Orthop Relat Res 2004;427:198-203. [Google Scholar] |
| 6. | Uda H, Mizuzeki T, Tsuge K. Osteoid osteoma of the metacarpal bone presenting after an injury. Scand J Plast Reconstr Surg Hand Surg 2002;36:238-42. [Google Scholar] |
| 7. | Kendrick JI, Evarts CM. Osteoid-osteoma: A critical analysis of 40 tumors. Clin Orthop Relat Res 1967;54:51-9. [Google Scholar] |
| 8. | Bednar MS, McCormack RR Jr., Glasser D, Weiland AJ. Osteoid osteoma of the upper extremity. J Hand Surg Am 1993;18:1019-25. [Google Scholar] |
| 9. | Baron D, Soulier C, Kermabon C, Leroy JP, Le Goff P. Post-traumatic osteoid osteoma. Apropos of 2 cases and review of the literature. Rev Rhum Mal Osteoartic 1992;59:271-5. [Google Scholar] |
| 10. | Healey JH, Ghelman B. Osteoid osteoma and osteoblastoma. Current concepts and recent advances. Clin Orthop Relat Res 1986;204:76-85. [Google Scholar] |
| 11. | Golding JS. The natural history of osteoid osteoma; with a report of twenty cases. J Bone Joint Surg Br 1954;36-B:218-29. [Google Scholar] |
| 12. | Sherman MS, Mcfarland G Jr. Mechanism of pain in osteoid osteomas. South Med J 1965;58:163-6. [Google Scholar] |
| 13. | Greco F, Tamburrelli F, Ciabattoni G. Prostaglandins in osteoid osteoma. Int Orthop 1991;15:35-7. [Google Scholar] |
| 14. | Basu S, Basu P, Dowell JK. Painless osteoid osteoma in a metacarpal. J Hand Surg Br 1999;24:133-4. [Google Scholar] |
| 15. | Carroll RE. Osteoid osteoma in the hand. J Bone Joint Surg Am 1953;35-A:888-93. [Google Scholar] |
| 16. | Wachtl SW, Exner GU, von Hochstetter A, Sennwald G. Osteoid osteoma of the hand. Case representation with special reference to magnetic resonance tomography and literature review. Z Orthop Ihre Grenzgeb 1995;133:76-8. [Google Scholar] |
| 17. | Towbin R, Kaye R, Meza MP, Pollock AN, Yaw K, Moreland M. Osteoid osteoma: Percutaneous excision using a CT-guided coaxial technique. AJR Am J Roentgenol 1995;164:945-9. [Google Scholar] |
| 18. | Ward WG, Eckardt JJ, Shayestehfar S, Mirra J, Grogan T, Oppenheim W. Osteoid osteoma diagnosis and management with low morbidity. Clin Orthop Relat Res 1993;291:229-35. [Google Scholar] |
| 19. | Adam G, Neuerburg J, Vorwerk D, Forst J, Gunther RW. Percutaneous treatment of osteoid osteomas: Combination of drill biopsy and subsequent ethanol injection. Semin Musculoskelet Radiol 1997;1:281-4. [Google Scholar] |
| 20. | Duda SH, Schnatterbeck P, Härer T, Giehl J, Böhm P, Claussen CD. Treatment of osteoid osteoma with CT-guided drilling and ethanol instillation. Dtsch Med Wochenschr 1997;122:507-10. [Google Scholar] |
| 21. | Gangi A, Dietemann JL, Guth S, Vinclair L, Sibilia J, Mortazavi R, et al. Percutaneous laser photocoagulation of spinal osteoid osteomas under CT guidance. AJNR Am J Neuroradiol 1998;19:1955-8. [Google Scholar] |
| 22. | de Berg JC, Pattynama PM, Obermann WR, Bode PJ, Vielvoye GJ, Taminiau AH. Percutaneous computed-tomography-guided thermocoagulation for osteoid osteomas. Lancet 1995;346:350-1. [Google Scholar] |
| 23. | Norman A. Persistence or recurrence of pain: A sign of surgical failure is osteoid-osteoma. Clin Orthop Relat Res 1978;130:263-6. [Google Scholar] |
| 24. | Voto SJ, Cook AJ, Weiner DS, Ewing JW, Arrington LE. Treatment of osteoid osteoma by computed tomography guided excision in the pediatric patient. J Pediatr Orthop 1990;10:510-3. [Google Scholar] |
| 25. | Vanderschueren GM, Taminiau AH, Obermann WR, Bloem JL. Osteoid osteoma: Clinical results with thermocoagulation. Radiology 2002;224:82-6. [Google Scholar] |
| 26. | Lindner NJ, Ozaki T, Roedl R, Gosheger G, Winkelmann W, Wörtler K. Percutaneous radiofrequency ablation in osteoid osteoma. J Bone Joint Surg Br 2001;83:391-6. [Google Scholar] |
Fulltext Views
2,106
PDF downloads
956




