Translate this page into:
Isolated anterior dislocation of the elbow in an adolescent
Corresponding Author:
Mohammed L S Alotaibi
Department of Surgery, College of Medicine, King Khalid University, P.O. Box: 641, Abha
Kingdom of Saudi Arabia
mohammedlafiotaibi@gmail.com
| How to cite this article: Alotaibi ML, Alfaya FF. Isolated anterior dislocation of the elbow in an adolescent. J Musculoskelet Surg Res 2020;4:163-165 |
Abstract
Although elbow dislocation is the most common dislocation in children, anterior elbow dislocation is considered to be rare. When it occurs rarely as an isolated elbow dislocation with no associated fractures. This report is about a case of isolated elbow dislocation with a rare mechanism of injury. A 14-year-old girl presented to the emergency department with an acute closed injury to her right elbow after her arm got caught and twisted in a washing machine. There was no associated neurovascular injury. A trial of closed reduction failed, so open surgical reduction was performed to avoid growth plate injury or fracture. Urgent open reduction was successful with a good outcome. Anterior elbow dislocation without fracture is a very rare injury and can occur with a vigorous twisting mechanism. Proper management is important to regain normal function. The aim of reporting this case is to emphasize that a rare isolated anterior elbow dislocation can occur by a twisting injury and an open reduction may be needed if a gentle closed reduction could not reduce it, to avoid growth plate injury in a skeletally immature patient.
Introduction
The elbow joint consists of three articulations; the ulnohumeral, the radiocapitellar, and the radioulnar articulations. The movements around the elbow include flexion and extension of the elbow joint, and pronation and supination of the forearm. The dislocation of the elbow can be anterior, posterior, lateral, or medial-based on the mechanism of injury.[1],[2] A fall on an outstretched hand is the most common mechanism of elbow dislocation.[3] The most common elbow dislocation is the posterior, whereas the rarest one is the anterior.[4],[5] The dislocations are usually associated with fractures of the medial epicondyle followed by the lateral condyle of the humerus.[1],[5] Most of the reported cases of anterior dislocation were associated with fracture of the olecranon process or distal end of the humerus.[1] It is even more rare to have an isolated anterior elbow dislocation without fracture in adolescents.[6]
The elbow is the most common joint to become dislocated in children.[5] The rate of elbow dislocations, among other elbow injuries in children, is 3%–6% annually.[7] Hyvönen et al. reported the rate of elbow dislocations in children between 1996 and 2014; the rate was 6.4 per 100,000 annually. Anterior dislocation reported in only 1.9% of the cases. The common injury mechanism of anterior elbow dislocation is a fall with a direct blow to the back of the elbow (olecranon). Falls off trampolines and snowboards are examples of such injuries.[8]
Case Report
A 14-year-old girl was admitted to the hospital with a history of trauma to her right elbow 2 h before presentation. Her right arm was caught and twisted vigorously in the roller of the washing machine while holding a wet blanket. The patient presented with severe pain, swelling, and deformity. She was holding her elbow in about 45° of flexion. The injury was closed with an intact neurovascular evaluation.
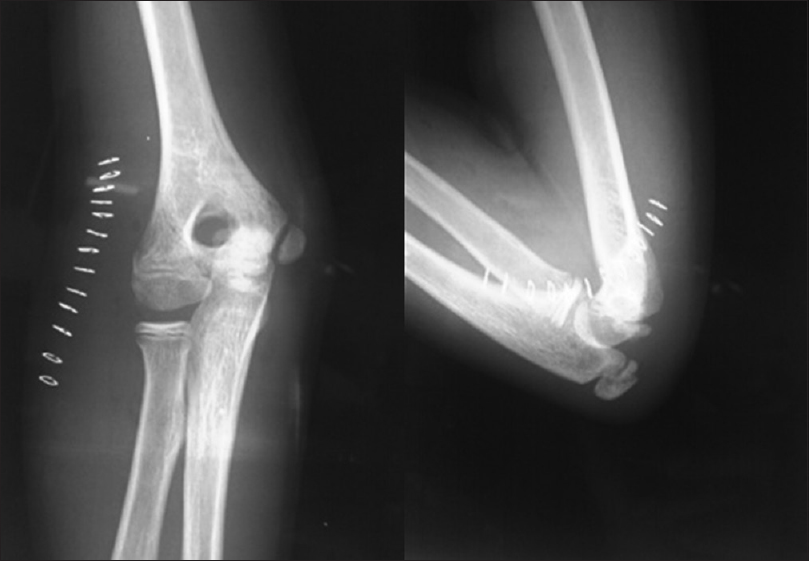
There was simple anterior elbow dislocation with no associated fractures, which is seen as anteromedial rather than anterior dislocation on anteroposterior and lateral radiographs, because positioning for proper radiograph was difficult due to pain [Figure - 1].
![[Figure - 1]](#fig_SaudiOrthopJ_2020_4_3_163_289107_f1.jpg){kind=link}
 |
| Figure 1: Radiographs of the right elbow showing isolated anterior elbow dislocation (no radio-ulna divergence indicating an intact annular ligament) |
Surgical technique
Under general anesthesia, a trial of gentle closed reduction of the elbow joint was not successful. Open reduction through the posterolateral (Kocher) approach was performed. Neurological preoperative examination as well as plain radiographs showing no radio-ulna divergence indicating an intact annular ligament, and the anterior interosseous nerve. There was complete peeling of the soft tissues from the distal part of the humerus with buttonholing through the triceps muscle and the anconeus facia [Figure - 2]. The elbow joint was reduced after the removal of the interposed triceps and anconeus muscles. It was clinically stable throughout the range of motion after reduction with no fractures or growth plate injuries [Figure - 3]. Repair of the lateral collateral ligament and the anconeus facia was carried out. Above elbow, The back slab in 90° of flexion and mid pronation position was applied and kept for 3 weeks to allow for soft-tissue healing. The patient was started on a self-assisted range of motion immediately after slab removal. She regained a functional range of motion the elbow within 3 months of rehabilitation.
![[Figure - 2]](#fig_SaudiOrthopJ_2020_4_3_163_289107_f2.jpg){kind=link}
![[Figure - 3]](#fig_SaudiOrthopJ_2020_4_3_163_289107_f3.jpg){kind=link}
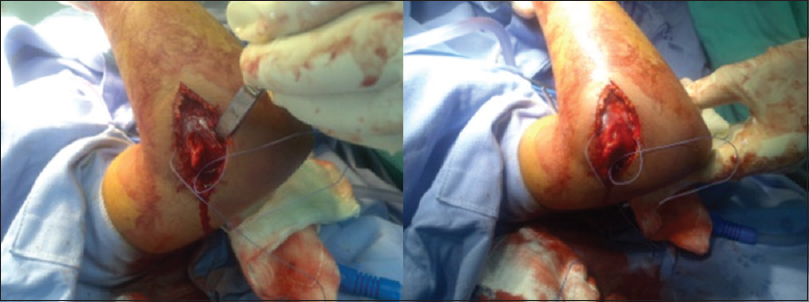 |
| Figure 2: A posterolateral approach used for the open reduction |
 |
| Figure 3: Postoperative radiographs (2 weeks) with congruent stable reduction of the elbow joint |
Discussion
In 1787, the first case of anterior elbow dislocation was reported by Evers.[9] Since then only few sporadic cases were reported in the literature. A direct blow to the back of the elbow (olecranon).[6] While in flexion is the most common mechanism of anterior elbow dislocation. In our case, the patient presented with an unusual mechanism of injury (vigorous twisting injury of the elbow). Among the rare cases with anterior dislocation, the case that was reported by Tees and McKim, in Montreal in 1923; they reported a patient with almost the same mechanism of injury with the arm caught between the rollers of a washing machine, although in that case the dislocation was associated with an olecranon fracture.[10]
The stability of the elbow depends on the primary stabilizers and secondary stabilizers. The primary stabilizers consist of bony articulation (ulno-humeral joint), the anterior band of the medial collateral ligament, and the lateral collateral ligament complex. The secondary stabilizers consist of the radiocapitellar articulation, the joint capsule, the common flexors and extensors origin, and the dynamic stabilizers. Disruption of the posterior column by fracturing the olecranon process is required to produce anterior dislocation.[11] This would explain the rarity of isolated anterior elbow dislocation.
By reviewing the literature, none of the cases reported as isolated anterior dislocation without a fracture. Carlioz and Abols reported that 64% of children with elbow dislocation had fractures in addition to the dislocation.[12] The elbow dislocation is usually anterior when there is an avulsion fracture of the olecranon process, as reported by Rasool.[1] The mechanism of an anterior elbow dislocation in association with an avulsion fracture of the olecranon process is usually caused by a direct blow to the posterior aspect of the elbow. The incidence of such injury is 1.9% of all elbow injuries in children and adolescents.[1],[8]
Most of the dislocations of the elbow in children are treated with closed reduction and splinting. Few cases may need to be operated on when closed reduction fails, associated with displaced fractures, unstable after reduction or neglected, and late presenting cases.[1],[8]
The outcome of closed reduction found to be better regarding regaining the elbow range of motion.[1] The closed reduction should be done gently to avoid growth plate injury, nerve entrapment, or fractures. In this case, open reduction was necessary and was successful.
To avoid stiffness of the elbow joint, it is recommended to start a range of motion and functional treatment as soon as possible.[13] This report is limited by the radiological short follow-up documentation, but the patient had full clinical recovery without complication.
Conclusion
Isolated anterior elbow dislocation can occur with a vigorous twisting injury of the arm. Early diagnosis and gentle, closed or open, concentric reduction of the joint and soft-tissue repair with early physiotherapy is required to regain the normal function of the elbow on the short-term follow-up.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient's parents have given their consent for her images and other clinical information to be reported in the journal. The parents understand that the patient's name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors..
Conflicts of interest
There are no conflicts of interest.
Authors' contributions
MLSA in charged of conceived, designed, conducted the research; analyzed and interpreted results of the work. FFA in charged for literature review. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
| 1. | Rasool MN. Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-8. [Google Scholar] |
| 2. | Sofu H, Gursu S, Camurcu Y, Yildirim T, Sahin V. Pure elbow dislocation in the paediatric age group. Int Orthop 2016;40:541-5. [Google Scholar] |
| 3. | Subasi M, Isik M, Bulut M, Cebesoy O, Uludag A, Karakurt L. Clinical and functional outcomes and treatment options for pediatric elbow dislocations: Experiences of three trauma centers. Injury 2015;46:14-8. [Google Scholar] |
| 4. | Polat G, Karademir G, Akgul T, Huseyin H, Akgul C. Pediatric open elbow dislocation without fracture: A case report. Int J Surg Case Rep 2014;5:1064-7. [Google Scholar] |
| 5. | Stans AA, Lawrence JT. Dislocations of the elbows, medial Epicondylar Humerus fractures. In: Flynn JM, Skaggs DL, Waters PM, editors. Rockwood and Wilkins' Fractures in Children. 8th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams &Wilkins; 2015. p. 625-98. [Google Scholar] |
| 6. | Borris LC, Lassen MR, Christensen CS. Elbow dislocation in children and adults. A long-term follow-up of conservatively treated patients. Acta Orthop Scand 1987;58:649-51. [Google Scholar] |
| 7. | Frongia G, Günther P, Romero P, Kessler M, Holland-Cunz S. Elbow dislocation in childhood. Long-term observational study. Unfallchirurg 2012;115:125-33. [Google Scholar] |
| 8. | Hyvönen H, Korhonen L, Hannonen J, Serlo W, Sinikumpu JJ. Recent trends in children's elbow dislocation with or without a concomitant fracture. BMC Musculoskelet Disord 2019;20:294. [Google Scholar] |
| 9. | Symeonides PP. Grigoriadis NC, Hatzokos IG. Anterior dislocation of the elbow. J Shoulder Elbow Surg 2006;15:249-51. [Google Scholar] |
| 10. | Tees FJ, McKim LH. Anterior dislocation of the elbow. Can Med Assoc J 1929;20:36-8. [Google Scholar] |
| 11. | Biga N, Thomine JN. Laluxariantrans-olecranienne du coude. Rev Chir Orthop 1974;60:557-67. [Google Scholar] |
| 12. | Carlioz H, Abols Y. Posterior dislocation of the elbow in children. J Pediatr Orthop 1984;4:8-12. [Google Scholar] |
| 13. | Lansinger O, Karlsson J, Körner L, Måre K. Dislocation of the elbow joint. Arch Orthop Trauma Surg 1984;102:183-6. [Google Scholar] |
Fulltext Views
4,465
PDF downloads
1,998




