Translate this page into:
Pattern and extent of traumatic epiphyseal injuries at Almadinah Almunawwarah
Corresponding Author:
Sultan Hatem Farsi
7390, Abu Burayqa, Almadinah Almunawwarah
Saudi Arabia
sulttan-1010@hotmail.com
| How to cite this article: Akhtar ZM, Farsi SH, Almahdi HH, Zahid A, Wali SM, Mohabbat AF, Mansi AK, Alghabban MM, Alrehaili OH. Pattern and extent of traumatic epiphyseal injuries at Almadinah Almunawwarah. J Musculoskelet Surg Res 2020;4:95-99 |
Abstract
Objectives: Epiphyseal plate is responsible for bone growth; hence, its preservation is vital for normal bone growth to occur. This study aimed to present the pattern of traumatic epiphyseal injury in a single regional hospital and list the most common causes of these injuries.Methods: This is a retrospective study, with a 1-year duration, started from October 30, 2017, using the hospital database of all admitted fracture cases for data collection at King Fahad Hospital, Almadinah Almunawwarah city, Saudi Arabia. Radiographs of all cases were reviewed. Epiphyseal injuries cases were included and classified using Salter–Harris (SH) classification.
Results: The 1-year prevalence of epiphyseal injury in this project was 7.8% out of 770 fractures. Falls were the most commonly incurred type of injury. Humerus was the most common fractured bone (48.3%), followed by radius (10%). Type II SH fracture was the most frequent type observed. Fractured bones and type were significantly related to the mechanism of injury, whereas gender and type of fracture were significantly related to the age group in years.
Conclusion: The 1-year prevalence of epiphyseal injuries in this study is moderately low. Falls were the most frequent mechanism of injury, and the humerus was the most commonly fractured bone, whereas SH Type II fracture was the most common morphology.
Introduction
Epiphyseal plate (growth plate) is a cartilaginous tissue in a skeletally immature bone that lies in between the epiphysis and metaphysis, which is responsible for growth. Hence, its preservation is vital for normal growth to occur.[1] The epiphyseal plate is considered the weakest part of the bone. This weakness increases with advancing age. In younger children, it is more cartilaginous, and it functions as a shock absorber; hence, torus fractures are usually more common.[1],[2] Epiphyseal fractures account for up to one-third of all pediatric fractures, being more common in males, with a peak incidence at 14 years of age in boys and 11 years of age in girls. This is probably due to the early closure of epiphyseal plates in girls in contrast to boys. Boys are exposed more to trauma as a result of athletic activities.[2],[3],[4] Upper limbs are the most commonly affected areas in both genders, with the distal radius being the most commonly affected area, followed by the ankle.[2],[3] Growth arrest in epiphyseal fractures happens in 5%–10% of the cases, and it depends on many variables such as trauma severity, mechanism of injury, location, time to diagnosed, treatment methods, and others.[2],[3],[5] Other complications that may occur as a result of an epiphyseal injury include permanent joint deformity and limitation of the joint movement and function, which may have a bad impact on the patient's quality of life.[2]
Throughout the years, the classification and assessment of epiphyseal injuries have passed through many changes. In 1885, before the invention of radiological imaging, the classification was only applicable to open fractures. The first international system was introduced by Poland.[6] Nowadays, we have many other systems for classification according to different measures, but the most commonly used one is the Salter–Harris (SH) classification, which is based on the anatomical structure of the epiphyseal injury and shows good predictive value for the prognosis and treatment of these fractures besides being easy to use.[7]
The importance of this study is due to the high prevalence of the growth disturbance associated with these types of injuries worldwide[8] and the lack of such studies in Saudi Arabia. There are many known causes of epiphyseal plate injuries. In this study, we focus on traumatic causes, which would help in preventing this kind of injury by increasing the society's awareness, and caution would be taken for preventable causes, from one side, and from the other side, increasing treating physicians' awareness so that patients can have proper diagnosis and management in time to reduce complications.
Although many epidemiological studies on epiphyseal injury were documented globally, this subject has not been fully discussed in Saudi Arabia.
Materials and Methods
This is a retrospective study done at King Fahad Hospital (KFH) in Almadinah Almunawwarah, Saudi Arabia, using the orthopedic department database and the hospital medical records for data collection. Inclusion criteria were all pediatric patients with traumatic epiphyseal injury, who presented to KFH over 1-year duration from October 30, 2017. The included age group was up to 14 years of age for females and 17 years of age for males based on the difference of age of the epiphyseal closure between genders.[4] Patients who presented with underlying bone diseases were excluded from the study. Cases with more than 10% missing data were excluded from the study. Data were collected using an electronic data-collecting sheet, including sociodemographic variables (such as age and gender) and the biomedical data (site, type, mechanism of injury, and SH classification). The radiographs were reviewed by a senior orthopedic resident using the SH classification to double-check the diagnosis for all the included cases. Statistical Package for Social Sciences (SPSS) version 21 (IBM Corporation, Armonk, New York, USA,) was used for data analysis. The relationship between the dependent and independent variables was calculated using Chi-square test. P ≤0.05 was accepted as a statistically significant level for all statistical tests. All the collected data were kept fully confidential without exposing any personal data related to the patients.
Results
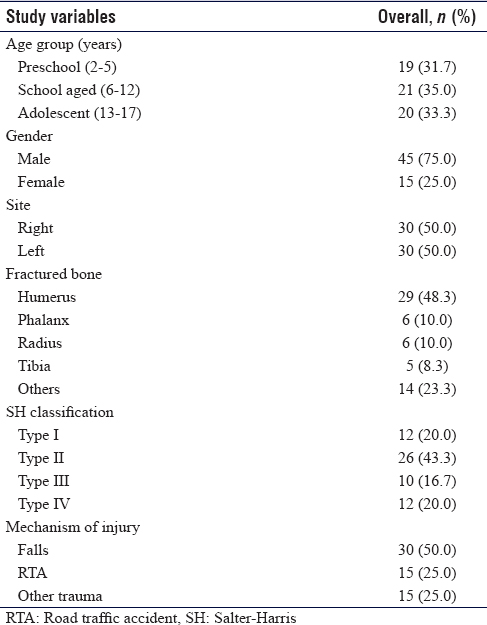
There were 770 pediatric cases with fractures admitted to KFH during the 1-year period of the study from October 30, 2017. Out of the 770 cases, 60 were identified as epiphyseal injuries, giving an overall prevalence of 7.8%. [Table - 1] presents the baseline characteristics of the patients with epiphyseal injuries. The age range was from 2 to 16 years (mean 9.1 ± 4.6 years standard deviation), with males accounting for 75% of the patients. The right and left sides were affected equally. Humerus was the most commonly fractured bone (48.3%), followed by radius (10%) and tibia (8.3%). With regard to the SH classification, Type II was the most common with 43.3%, followed by Type I and Type IV SH with 10% for each. Isolated medial and lateral condylar humerus fractures accounted for 16.7% and 13.3%, respectively, whereas the most frequent mechanism of injury was falls (30%).
![[Table - 1]](#tbl_SaudiOrthopJ_2020_4_2_95_280597_t1.jpg){kind=link}
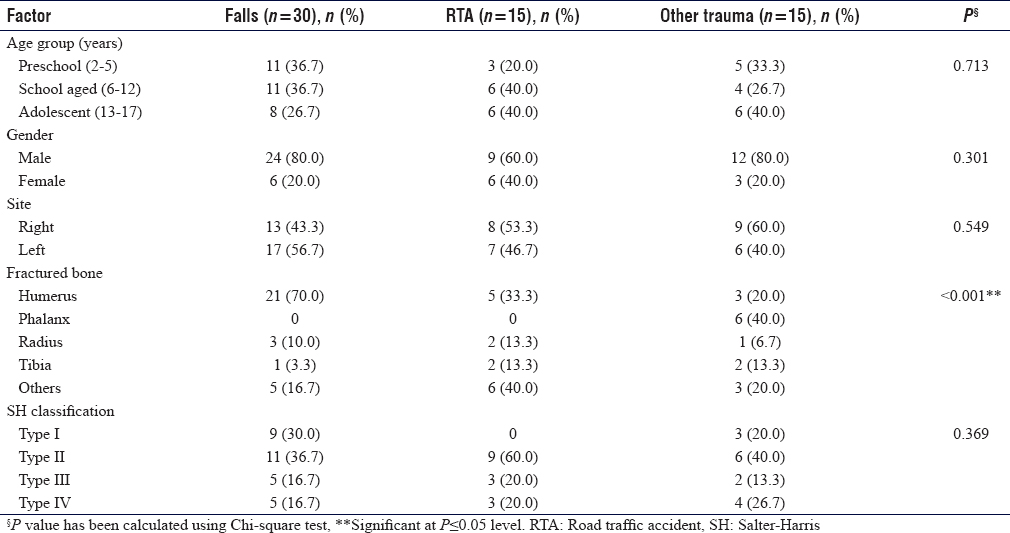
It was found that patients with falls have statistically significantly more chances of having physeal injuries with an overall percentage of 50% followed by road traffic accidents (RTA) and other types of trauma (twisting, crushing, and blunt trauma resulting from fighting and hitting) with 25% each (P < 0.001).
We also found that Type IV SH injuries were statistically significantly higher in RTA, whereas medial and lateral condyles were more in fall injuries (P = 0.003).
We also found that age, gender, site, and SH classification have no significant relationship with the mechanism of injury [Table - 2].
![[Table - 2]](#tbl_SaudiOrthopJ_2020_4_2_95_280597_t2.jpg){kind=link}
[Table - 3] shows that epiphyseal injuries in males have a statistically significant relationship with age with preschool children, school-aged children, and adolescents; 90%, 57.1%, and 78.9%, respectively (P = 0.047).
![[Table - 3]](#tbl_SaudiOrthopJ_2020_4_2_95_280597_t3.jpg){kind=link}
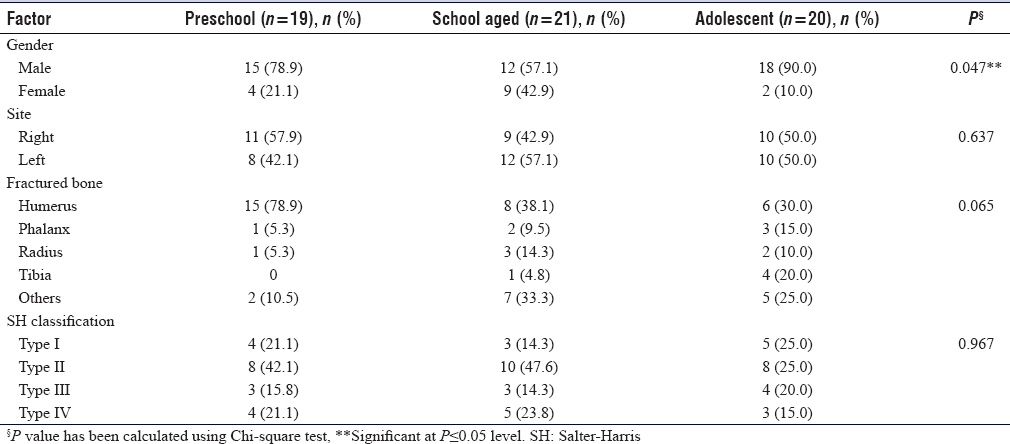
Although there was no statistically significant relationship, we found that humerus was the most commonly fractured bone in preschoolers (P = 0.065). However, Type II SH fracture was higher across all age groups (P = 0.967).
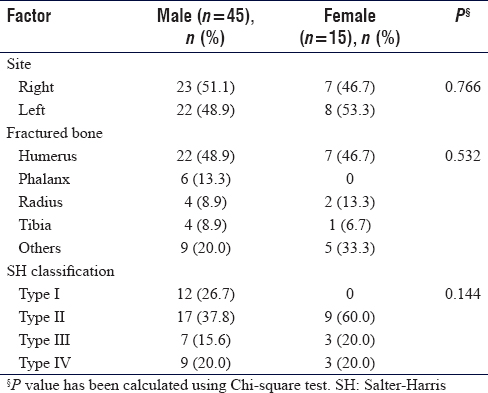
When we observed the relationship between gender and the baseline characteristics of patients, site of the fracture, fractured bone, the exact part of the fracture, and SH type, we found no significant relationship with gender [Table - 4].
![[Table - 4]](#tbl_SaudiOrthopJ_2020_4_2_95_280597_t4.jpg){kind=link}
Discussion
In this study, the prevalence of epiphyseal injury for a 1-year period was 7.8%. This is lower than what was reported in a Japanese study in pediatric fractures (17.9%).[9] Although their prevalence was based on a 5-year period, the sample size was relatively larger compared to our study. In Scotland, the incidence of traumatic epiphyseal injuries was also higher, with 14.8% among 2198 cases in a 1-year duration.[10] Binder et al. reported a prevalence of 23.4% (only epiphyseal injuries associated with proximal humerus fractures) among 303 cases.[11] On the contrary, Verlinden and Lewis reported only 1.2% (12 cases) of epiphyseal trauma among 961 skeletons with open physis (0–17 years).[12]
In this study, most cases of epiphyseal injuries were due to falls (50%) followed by RTA and other types of trauma, with 25% for each. In literature, the mechanism of injury differed across the regions.[8],[10] Caine cited that football was the sport most frequently attributed to chronic epiphyseal injuries among American children.[8] In Japan, the main cause of epiphyseal injuries was athletic exercises followed by falls. While in Scotland, the most common causes of epiphyseal injuries were falls and blunt trauma.[9],[10]
This study also documents that the humerus was the most commonly fractured bone (48.3%), and complex distal humerus epiphyseal injury Type IV SH (20%) and isolated medial and lateral condyles with 16.7% and 13.3%, respectively, were found to be the most common specific forms of fractures among the included cases. Verlinden and Lewis found that epiphyseal injuries occurred predominantly at the distal end of humerus, which was consistent with our study findings.[12] Kawamoto et al. reported that the phalanges of hands and lateral condyle humerus fractures were the most frequently injured among children treated with limb injuries.[9] This has been supported by a study published by Rennie et al., as they reported that the most common site to get a fracture was the distal radius and phalanges of the fingers. In a study published by Dover and Kiely, they found that the distal radius was the most common site of fractures in children, whereas the ankle was the second most common site of epiphyseal injury, with high complication rates.[1]
Regarding the SH classification, the most common type was Type II (43.3%), followed by Type I and Type IV (20% each). Several published studies reported SH Type II to be the most common type of epiphyseal injury.[3],[9],[11] Mallick and Prem reported Type II as the most common SH pattern, whereas Type I accounted for only 6% of all epiphyseal injuries in their series. They further elaborated that Type I is rare and can be seen usually in infants and commonly involve the proximal or distal humerus and the distal femoral physis but can also be observed in the distal radius.[3] Kawamoto et al. reported that SH Type II revealed the largest number of cases among other types (60.9%) followed by Type I (28.6%), which was a slightly higher incidence compared to our study.[8] In Austria, 58.3% of patients presented with an SH Type II injury followed by 31.9% of Type I.[11] In addition, another published article in Austria showed that Type II injuries were seen in 58% of patients, followed by Type III with 33.8%.[11]
Consequently, this article revealed that those patients who sustained an injury from falls had higher chances of having humeral fractures. We further noticed that cases of RTA and other forms of trauma are more associated with complex distal humerus epiphyseal Type IV SH and isolated medial and lateral condyles fractures. In addition, we also documented that males were predominantly affected with epiphyseal injuries compared to females, and the cases increased during the adolescent period (13–17 years old). In the United Kingdom, they reported that mechanisms of injury, which were associated with sprains and dislocations in adults, were associated with epiphyseal injury in children.[1]
Chronic and severe epiphyseal injuries can lead to complications. Injury to the epiphyseal plate often stimulates bone repair, which can lead to bone bridge formation between the metaphysis and epiphysis, leading to angulation and shortening of the bone.[1] Although in this study, the detailed description of complications was not collected, it is of importance to note the potential complications of epiphyseal fracture.
Limitations
The study limitation include not being able to apply the research to all hospitals in Almadinah Almunawwarah due to the different hospital regulations and administrative rules, though KFH is the main referral hospital in the region where the majority of cases are treated. Also, some cases were excluded due to lack of proper documentation in the system as well as some data, which could have been beneficial to the study, were missed from the files such as weight and height. The study included only patients who were admitted to the hospital for surgical management, which excluded many cases treated conservatively without admission. Furthermore, SH Type V was not included as it is not diagnosed during the first admission.
Conclusion
The 1-year incidence of epiphyseal injury in this study is moderately low compared to the literature. Falls were the most frequent mechanism of injury, and humerus was the most commonly fractured bone, whereas SH Type II fracture was the most common type. Moreover, fractured bone and the exact fractured part are significantly related to the mechanism of injury.
Recommendation
It is important to predict and notice epiphyseal injuries in order to give the best management to prevent or decrease possible complications. Further researches with larger samples are needed in order to validate the pattern and extent of traumatic epiphyseal injury in our country.
Ethical consideration
Ethical approval was obtained from the research ethical committee of KFH.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Author's contributions
ZMA conceived and designed the study, organized and reviewed drafts. SHF, contribute to the conception and design of the work, corresponding to the journal with the editing, provided research materials and logistics. HHA and AZ interpreted data, radiographs and finalize the work. SMW, AFM, AKM, MMA, OHA conducted research and analyze the data. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
| 1. | Dover C, Kiely N. Growth plate injuries and management. Orthop Trauma 2015;29:261-7. [Google Scholar] |
| 2. | Dodwell ER, Kelley SP. Physeal fractures: Basic science, assessment and acute management. Orthop Trauma 2011;25:377-91. [Google Scholar] |
| 3. | Mallick A, Prem H. Physeal injuries in children. Surgery 2017;35:10-7. [Doi: 10.1016/j.mpsur. 2016.10.0]. [Google Scholar] |
| 4. | Peterson HA. Epiphyseal Growth Plate Fractures. Springer-Verlag, Berlin, Heidelberg; 2007. [Doi.org/10.1007/978-3-540-33802-4]. [Google Scholar] |
| 5. | Lidder S, Ramachandran M. Epiphyseal growth-plate injuries. In: European Surgical Orthopaedics and Traumatology: The EFORT Textbook. Springer-Verlag, Berlin, Heidelberg; 2014. p. 4653-68. [Google Scholar] |
| 6. | Poland J. Traumatic Separation of the Epiphyses. London: Smith, Elder; 1898. [Google Scholar] |
| 7. | Salter RB, Harris WR. Injuries involving the epiphyseal plate. J Bone Joint Surg 1963;45:587-622. [Google Scholar] |
| 8. | Caine DJ. Growth plate injury and bone growth: An update. Pediatr Exerc Sci 1990;2:209-29. [Google Scholar] |
| 9. | Kawamoto K, Kim WC, Tsuchida Y, Tsuji Y, Fujioka M, Horii M, et al. Incidence of physeal injuries in Japanese children. J Pediatr Orthop B 2006;15:126-30. [Google Scholar] |
| 10. | Rennie L, Court-Brown CM, Mok JY, Beattie TF. The epidemiology of fractures in children. Injury 2007;38:913-22. [Google Scholar] |
| 11. | Binder H, Schurz M, Aldrian S, Fialka C, Vécsei V. Physeal injuries of the proximal humerus: Long-term results in seventy two patients. Int Orthop 2011;35:1497-502. [Google Scholar] |
| 12. | Verlinden P, Lewis ME. Childhood trauma: Methods for the identification of physeal fractures in nonadult skeletal remains. Am J Phys Anthropol 2015;157:411-20. [Google Scholar] |
Fulltext Views
1,363
PDF downloads
200




