
Translate this page into:
Surgical treatment of flexible flatfoot in adolescents: Sinotarsic endorthesis
 MD., Lawrence Camarda1MD., Ludovico Lucenti1,MD.
MD., Lawrence Camarda1MD., Ludovico Lucenti1,MD.
*Corresponding author: Ludovico Lucenti, Department of Precision Medicine in Medical, Surgical and Critical Care (Me.Pre.C.C.), University of Palermo, Palermo, Italy. ludovico.lucenti@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Manuri V, Moscadini S, Salmeri L, Miceli A, Camarda L, Lucenti L. Surgical treatment of flexible flatfoot in adolescents: Sinotarsic endorthesis. J Musculoskelet Surg Res. 2025;9:76-83. doi: 10.25259/JMSR_217_2024
Abstract
Objectives:
The surgical procedure of arthroereisis for flexible flatfoot involves placing a screw or spacer between the talus and calcaneus, limiting the excessive inclination of the calcaneus. This study aimed to evaluate the clinical results of patients treated using an endosenotarsal screw.
Methods:
Seventy-three patients were treated with arthroereisis (54 unilateral and 19 bilateral) using the Fit-As subtalar screw (Gemes®). A total of 92 screws were implanted. Pre- and post-operative clinical evaluations were performed before and 3 months after the operation.
Results:
The median follow-up period was 46 months (12–80 months). The average age at the time of surgery was 12 years (range 8–19 years). The mean pre-operative American Orthopedic Foot and Ankle Society (AOFAS) score was 63.7/100, while the mean post-operative AOFAS score was 98.6/100. The average pre-operative disability index Foot and Ankle Disability Index Questionnaire was 77.7/104, whereas the average post-operative index was 102.3/104. None of the treated patients required surgical screw removal at the time of the final follow-up.
Conclusion:
The results obtained in this series of patients with Fit-As titanium endorthesis are in accord with those reported in the literature and lead to good clinical results, the absence of complications, and the unnecessary removal of the device.
Keywords
Adolescents
Arthroereisis
Calcaneo-stop
Endorthesis
Flatfoot
Pes planovalgus

INTRODUCTION
Flexible flatfoot (also known as pes planovalgus) is a morphologic modification of the foot characterized by a reduction in the plantar arch, sometimes related to hindfoot valgus.[1,2]
In a flatfoot, detorsion of the plantar helix along the longitudinal hinge, constituted by the functional articulation between the talus and calcaneus, is detected, leading to altered foot anatomy. This condition is clinically characterized by:
Heel valgus with pronation of the cuboid;
Inferomedial descent of the talar head, which is associated with synchronous displacement of the navicular and the three medial rays.[3,4]
The plantar vault is formed through a re-alignment process of the talocalcaneal joint. The foot has a physiological valgus of the hindfoot that can reach 12–15 from birth to 12 months. This valgus angle stabilizes to around 5–7 by the 5th year, eventually reaching a “normal” valgus position of the hindfoot, which is <5 on completion of the maturation process. A flatfoot deformity can occur when this process is troubled due to intrinsic or extrinsic factors.[3,4]
In 95% of cases, a certain degree of flatness is considered physiological at the age of 3 years, often referred to as “loose foot.” In these instances, there is a potential for spontaneous correction, with the foot progressing toward definitive maturation and regular support by the age of 6–8 years. This necessitates ongoing monitoring over time. Only 5% of cases will develop into idiopathic pathological flatfoot.[3,4]
The clinical classification divides flatfoot into rigid or flexible based on the mobility of the subtalar or other tarsal joints.[5,6] Furthermore, based on the relationship between the isthmus and the entire area of the foot at the podometric examination, this pathology can be divided into 3 [Figure 1]:
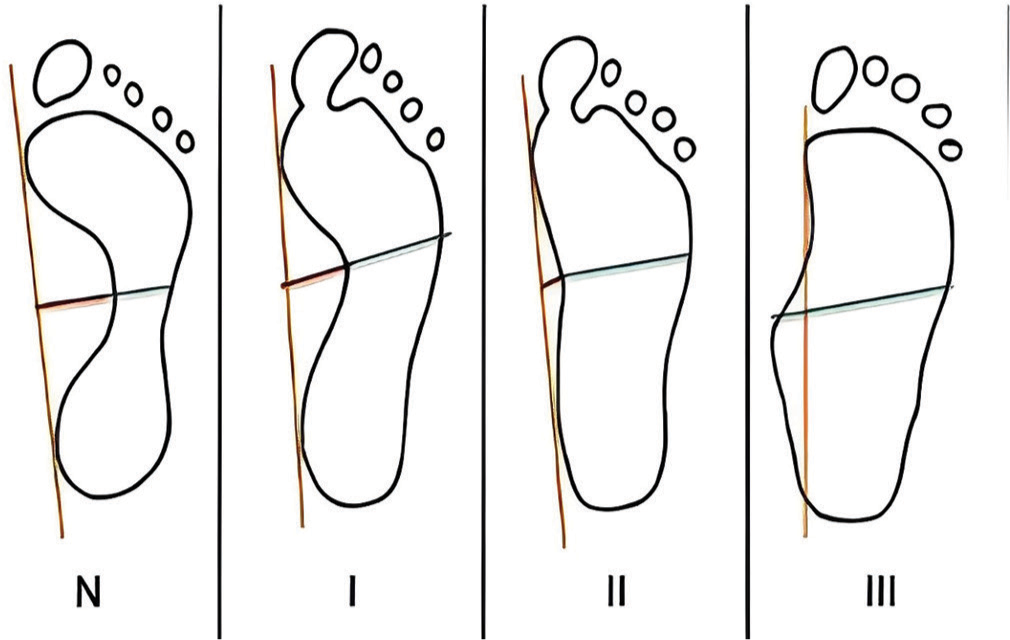
- Degrees of flatfoot. N: Footprint is normal, I: Plantar arch reduced but still present, the width of the midpart of the foot is between 1/2 and 1/3 of the width of the anterior part, II: The width of the midpart of the foot is between 2/3 and the entire width of the heel, III: Plantar arch completely absent, the isthmus is beyond the width of the heel.
1st: between 1/3 and 2/3
2nd: between 2/3 and the entire width of the heel
3rd: beyond the width of the heel.[7]
From a radiological point of view, Meary’s angle is evaluated: the angle, that is, between the talus and the first metatarsal in the latero-lateral projection of the foot [Figure 2].

- Meary’s angle.
In the physiological foot, Meary’s angle is a straight line between the talus and the first metatarsal, with a relative angle of 180 . On the other hand, in the pronated valgus foot, it forms two consecutive lines with a lower convex angle.[7]
Over the years, various surgical corrections have been proposed for the treatment of flexible flatfoot in adolescents. They include soft-tissue procedures (e.g., tendon transfers), re-alignment osteotomies, arthrodesis, and range of motion (ROM) non-limiting techniques without bone fusion (e.g., arthroereisis)[8] [Table 1].
| Procedure | Description | Pros | Cons |
|---|---|---|---|
| Soft tissue procedures | Achilles lengthening to improve ankle range of motion Tendon transfers to realign muscular forces across the foot |
May be used as adjunct with other procedures | Less efficacy when performed in isolation |
| Osteotomy | Cutting and realigning bones to correct pathologic alignment | A powerful surgery that offers large corrective capabilities Reliable outcomes when performed correctly |
Relies on bone healing to maintain correction Possibility of overcorrection |
| Arthrodesis | Fusion of joint to reduce motion and maintain joint alignment | Provides definitive correction Very powerful correction |
Irreversible elimination of joint movement Degeneration of adjacent joints Only used as last resort for children with physiologic flatfoot |
| Arthroereisis | Insertion of metal, silicone, or biodegradable implant into talocalcaneal joint | Minimally invasive implant may be removed Does not alter bony or muscle anatomy |
True long-term corrective ability unknown |
Arthroereisis is a non-fusion technique designed to limit the ROM without completely abolishing it. First introduced in the mid-1900s, this procedure involves the implantation of a metal, plastic, or bioabsorbable device within the sinus tarsi (endosenotarsal) or between the talus and calcaneus (extrasenotarsal). This device restricts excessive eversion of the subtalar joint, thereby preventing the collapse of the foot arch. The procedure is less invasive as it does not require osteotomies.[9,10]
Complications such as malpositioning of the implant, improper corrections, loosening of the implant, intolerance to fixation devices, fibular spasms, and persistent pain have been reported. These complications can be treated by removing the endorthesis. More serious complications include fractures of the talar neck and the development of a subtalar fusion. However, many documented cases of osteoarthritis show favorable radiographic findings and improved foot alignment.[8]
Furthermore, when it is chronic or not treated, it can result in unwanted long-term sequelae affecting the entire lower limb.[5] The early approach to flatfeet implicates conservative procedures, such as rest, anti-inflammatories, physical therapy, and orthotics; surgical intervention is reserved for children who have symptoms and are either over 8 years of age or do not respond to conservative treatment.[11]
Various surgical corrections have been suggested, often depending on the geographical area of reference. In Western and Southern Europe, the arthroereisis procedure is more widespread. The operating process involves placing a screw or spacer between the talus and calcaneus, restricting the extreme inclination of the calcaneus.[12] The surgical wound is very short, and functional recovery is rapid. The present study aimed to evaluate the clinical results of consecutive patients treated for flatfoot with arthroeresis using an exosinotarsal device.
MATERIALS AND METHODS
All patients were affected by idiopathic flexible and symptomatic pronated valgus flatfeet with or without associated foot or lower limb deformities such as juvenile hallux valgus, short Achilles tendon, and knee valgus.[13]
Inclusion criteria were as follows: Skeletal immaturity with growth cartilage visible on pre-operative foot radiographs; flexible flatfoot deformity; and symptoms (pain, reduced function, and/or limitations) not responsive to conservative treatment.
The exclusion criteria were as follows: Body mass index (BMI) >30, age <8 years and over 20 years, and association with other rigid deformities such as tarsal synostosis, arthritic pathologies, joint stiffness, and neurological pathologies characterized by ligament laxity, congenital or post-traumatic flatfoot, diabetes, or immunological diseases. The primary demographic and clinical data were recorded, including sex, underlying pathologies, age at surgery, operated side, BMI, type of surgery, any concomitant procedures carried out, and the duration of follow-up [Table 2].
| Patients | 73 Patients 92 Implants |
54 unilateral implants 19 bilateral implants |
| Sex | 29 females 44 males |
|
| Average Age | 12 years old | 8 years old min. 19 years old max. |
| Follow-up | 46 months | 12 months min. 80 months max. |
Pre- and post-operative clinical evaluations were performed before the operation. Three months after surgery, using the American Orthopedic Foot and Ankle Society’s (AOFAS) Scale for ankle and hindfoot (Italian version validated by the Italian Foot Surgery Society),[14] and the Foot and Ankle Disability Index (FADI) Questionnaire [Figures 3 and 4].[15] The AOFAS scale for ankle and hindfoot score comprises nine items organized into three categories: Pain (40 points), functional aspect (50 points), and alignment (10 points), summing up to a total of 100 points.[14] Patients responded to items related to pain and functional limitation, while an examiner evaluated the alignment items. The FADI is a self-report tool designed to assess the function. It encompasses 34 items categorized into two subscales. The first subscale comprises 26 items addressing activities of daily living (ADL) and pain, while the second subscale includes eight items focusing on sports activities. Each item is evaluated using a five-point Likert scale (4–0). Subsequently, the scores are transformed into percentages. Scores for the ADL and sports subscales are calculated independently.[15]
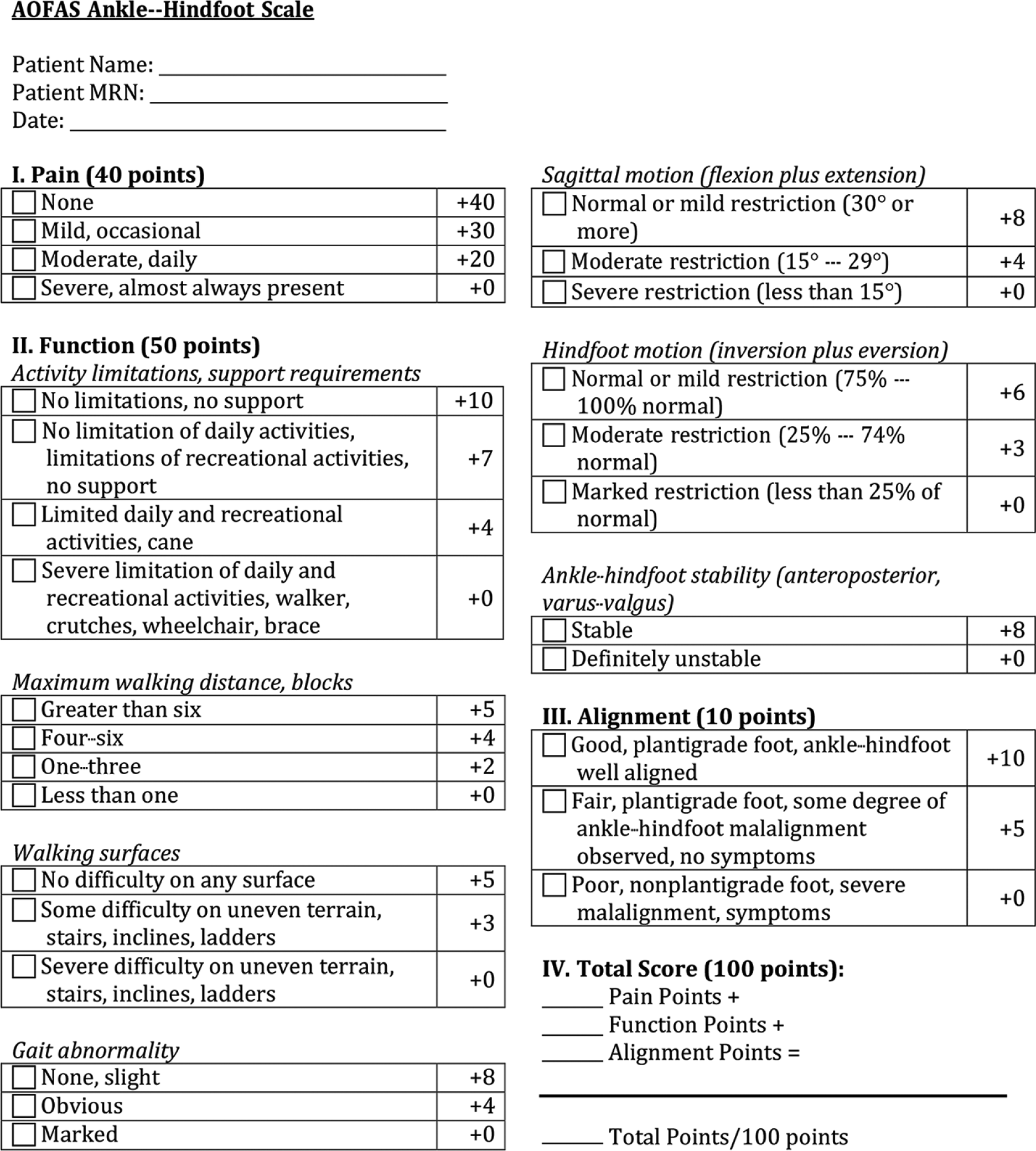
- American orthopedic foot and ankle society (AOFAS) score.
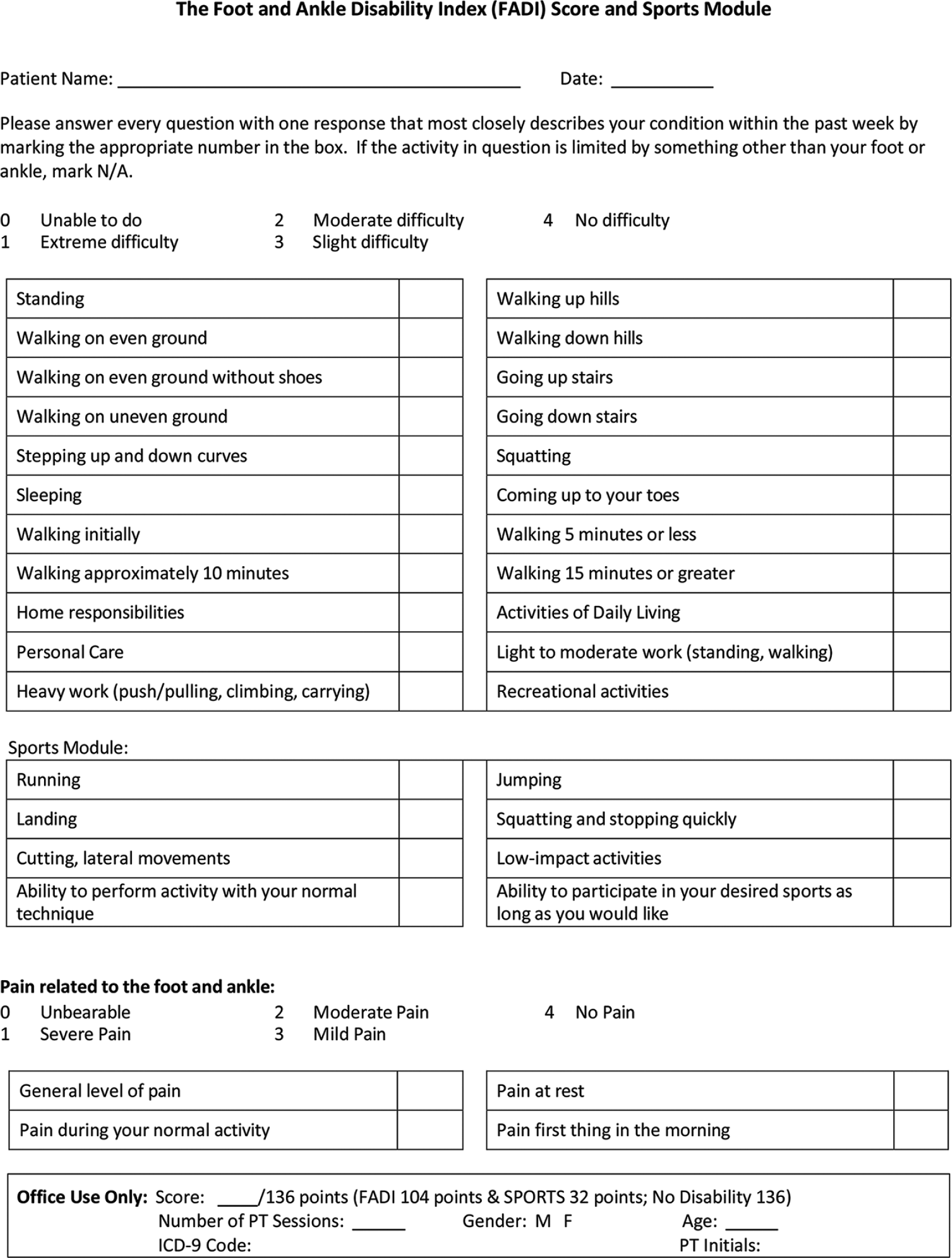
- Foot and ankle disability index (FADI) questionnaire.
Surgical technique
One surgeon, trained in foot and ankle surgery, performed all the surgeries. Under antibiotic prophylaxis, all patients were treated with local anesthesia using 5 mL of lidocaine hydrochloride 20 mg/mL associated with intravenous sedation and analgesia. Patients were placed in a supine position on the operating table without a hemostatic tourniquet. A 1 cm skin incision was made at the level of the sinus tarsi. A guide wire was inserted between the talus and the calcaneus, and on this, a trial endorthesis was placed until good alignment was clinically observed. At this point, the definitive screw was inserted [Figure 5]. Post-operatively, immediate full-weight bearing was allowed. If Achilles tendon lengthening and tibialis posterior re-tensioning were performed, non-weight bearing was suggested, and a cast was maintained for 3 weeks.

- (a) Surgical technique. Approximately 2 cm incision centered on the sinus tarsi in the line passing between the fibular malleolus and the cuboid, (b) A lateral view of the screw inserted in the sinus tarsi.
Radiographic assessment
All patients underwent a pre-operative radiographic evaluation with Meary’s angle assessment. Meary’s angle is determined by the relationship between a line traced along the longitudinal axes of the talus (mid-talar axis) and the first metatarsal (first metatarsal axis). This angle, also known as the talus-first metatarsal angle, is employed in assessing the severity of pes planus through lateral weight-bearing foot radiographs.[7]
RESULTS
Between November 2015 and September 2022, 512 consecutive patients underwent surgery for flatfoot. Of these, 73 patients were treated with arthroereisis (54 unilateral and 19 bilateral) using the Fit-As subtalar screw (Gemes®) [Figure 6]. Twenty-nine females and 44 males were treated surgically. A total of 92 screws were implanted in these patients.
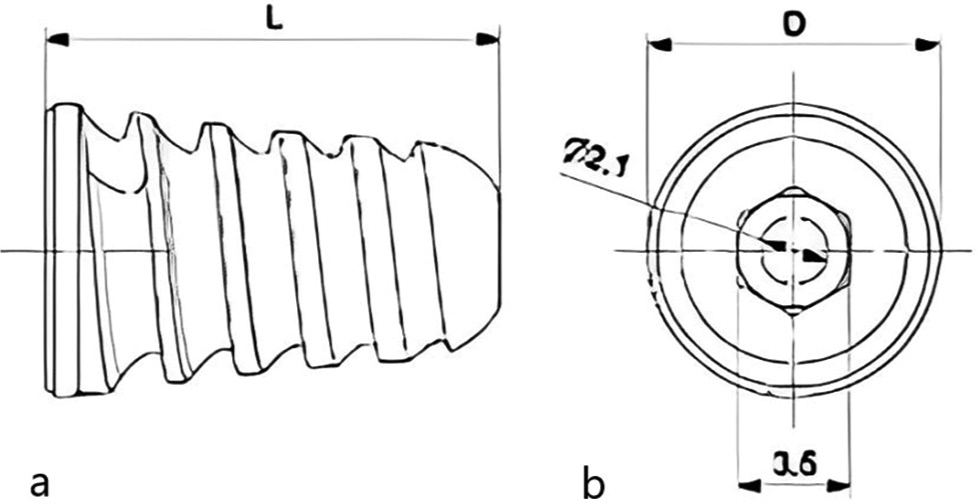
- The screw used for arthroereisis procedure: (a) View of the screw at its maximum length, (b) View of the screw and its diameter.
The main follow-up period was 46 months (12–80 months). The average age at the time of surgery was 12 years (range 8–19 years). No complications were observed, such as dehiscence of the surgical wound, early intolerance of the fixation implant, displacement of the fixation implant, or infections. Other complications, such as pain in the surgical scar, local symptoms at the incision, screw loosening, and contracture of peroneal muscles, were not reported.
A statistical improvement was noted when comparing pre- and post-operative scores. Specifically, the mean pre-operative AOFAS score was 63.7/100, while the mean post-operative AOFAS score was 98.6/100. The average pre-operative disability index (FADI Questionnaire) was 77.7/104, whereas the average post-operative index was 102.3/104 [Figure 7]. None of the treated patients required surgical screw removal at the time of the final follow-up.
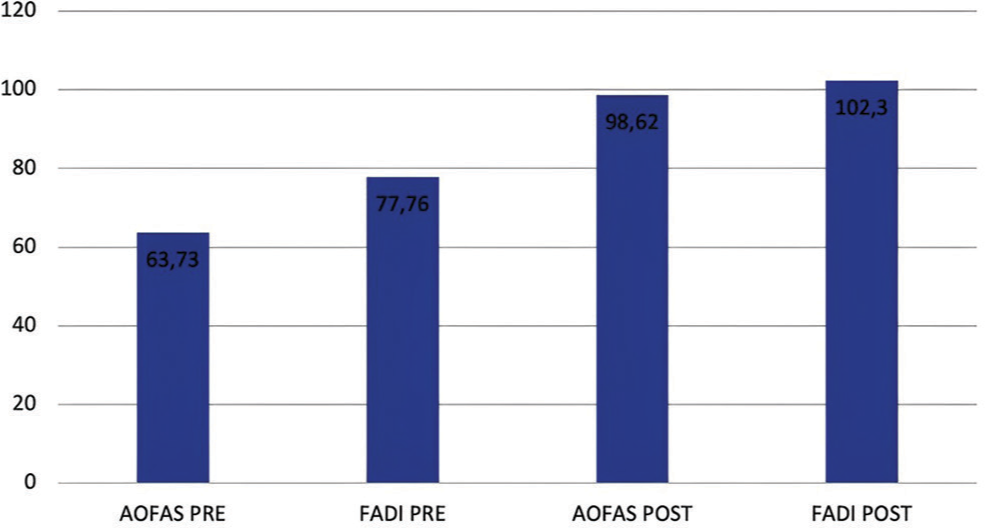
- Results of the scores. AOFAS: American orthopedic foot and ankle society, FADI: Foot and ankle disability index.
DISCUSSION
The flatfoot is a morphological alteration of the foot characterized by a decrease in the plantar arch, associated or not with the presence of hindfoot valgus.[1,2] There are numerous evidence in the literature in favor of correcting flexible flatfoot with the use of absorbable and nonabsorbable subtalar endorthesis.[16] In the studies by Giannini et al.,[9,17] as early as 1 year after the intervention, recovery of joint excursion, foot stability in monopodial stance, rapid clinical and radiographic improvement, a significant reduction in the pronator moment of the tibiotarsus foot complex during walking, and earlier normalization of load absorption and propulsion abilities were observed. This technique, according to other authors,[3,4,12,18] is easy to perform, less traumatic, and has a short hospitalization time, warranting easily manageable post-operative pain and sparing of endosinotarsal proprioceptive structures, as the joint is not damaged.
However, the chance of further removal of the screw must be considered once the correction has taken place and stabilized or in the event of intolerance to the fixation devices. In many cases, the decision is made to carry out the operation in a bilateral and contemporary way. In the experience conducted by Moscadini et al.,[19] it was observed that this led to symmetrical neuromotor re-coordination and reduction of psychophysical traumas due to deferred operations.
The experience we reported in the treatment of flexible flatfoot with endorthesis is largely positive, considering the excellent results obtained on the evaluation scales: The resulting average value of the post-operative AOFAS score was 98.62/100, compared to a pre-operative value of 63.73/100. The average disability index given by the FADI questionnaire went from 77.76/104 to 102.30/104.
The main limitations of the scales are the non-specificity and high subjectivity of the pathology in question. In addition, post-operative radiographic controls demonstrate a normalization of Meary’s angle.
As reported in other studies,[3,12] compared to other surgical techniques for treating flatfoot, this technique offers several advantages. The brief surgical duration (approximately 10 min per foot) minimizes the risk of infection and anesthesia-related complications. Conducting the procedure under assisted local anesthesia facilitates rapid post-operative recovery and significantly reduces the likelihood of adverse effects associated with anesthesia. It also allows the patient to be discharged on the same day. The simple surgical technique, minimally invasive concerning the anatomical structures without altering the foot’s morphology, allows easy reproducibility and a rapid learning curve.
In our experience, the use of intraoperative fluoroscopy has been retained only for the first cases as it is not necessary once the technique has been mastered, thus avoiding exposure to ionized radiation for adolescent patients [Figure 8]. The operation can also be performed bilaterally in the same operating session and with the same anesthetic indications.

- Post-operative radiographs: (a) AP view, (b) Oblique view, (c) Lateral view.
Compared to other techniques, this results in short healing times, early concession of the load, absence of plaster immobilizations, unless concurrent ancillary procedures were performed as well on the soft tissues, early resumption of normal daily and social activities, rapid hospitalization, and considerable reduction of health costs.
Biologically inert titanium synthetic devices guarantee the absence of reactive inflammation in the post-operative follow-up, immediate talocalcaneal alignment, and block of calcaneal valgus under load without affecting joint functionality, characterized by better tolerability even compared to absorbable materials.[16,20]
Pain reduction occurs quickly with the possibility of immediate loading, allowing rapid adaptation to the new proprioceptive and nociceptive structure with little recourse to common analgesics.
The results obtained in this series of patients with FitAs titanium endorthesis align with those reported in the literature. They are characterized by the absence of complications and the unnecessary removal of the device.[12]
This study has some limitations. First, it included 73 patients, which is a limited sample size. It was conducted at a single institution and by a single surgeon, which may limit the applicability of the findings to other contexts. A larger cohort and a multicenter study would provide more robust data. The study is retrospective, and the absence of a control group, such as patients treated conservatively or with other surgical procedures, limits the study’s results. The follow-up period ranged from 12 to 80 months, with a median of 46 months. It provides a good medium-term perspective, but longer follow-up and potential late-onset complications of the procedure were not investigated.
CONCLUSION
The use of Fit-As titanium endorthesis seems to be effective and safe for the treatment of flexible flatfoot in adolescents, with significant improvements in clinical outcomes, low risk of complications, and the advantages of a minimally invasive approach.
RECOMMENDATIONS
To validate this study’s findings, multicenter studies with larger sample sizes, an extended follow-up period, and a comparison with other conservative or surgical techniques are necessary.
AUTHORS’ CONTRIBUTIONS
Conceptualization, LC, VM, and SM; methodology, LC, VM, and LL; formal analysis, AM, LS; investigation, SM, AM; resources, VM; data curation, AM and VM; writing – original draft preparation, VM, LL and LC; writing – review and editing, LL, VM, LS, and LC; visualization, and SM; supervision, LC. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
ETHICAL APPROVAL
This study protocol was reviewed and approved by the Ethical Committee of the University Teaching Hospital of Palermo. (No. 1017 - 19.07.2023).
DECLARATION OF PATIENT CONSENT
Informed consent was waived per institutional protocol.
USE OF ARTIFICIAL INTELLIGENCE (AI)-ASSISTED TECHNOLOGY FOR MANUSCRIPT PREPARATION
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Flatfoot deformity in children and adolescents: Surgical indications and management. J Am Acad Orthop Surg. 2014;22:623-32.
- [CrossRef] [PubMed] [Google Scholar]
- Pathology and management of flexible flat foot in children. J Orthop Sci. 2019;24:9-13.
- [CrossRef] [PubMed] [Google Scholar]
- Results of the Italian pediatric orthopedics society juvenile flexible flatfoot survey: Diagnosis and treatment options. J Pediatr Orthop B. 2022;31:e17-23.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and treatment of flexible flatfoot: Results of 2019 flexible flatfoot survey from the European Paediatric Orthopedic Society. J Pediatr Orthop B. 2021;30:450-7.
- [CrossRef] [PubMed] [Google Scholar]
- A guide to the management of paediatric pes planus. Aust J Gen Pract. 2020;49:245-9.
- [CrossRef] [PubMed] [Google Scholar]
- Non-surgical interventions for paediatric pes planus. Cochrane Database Syst Rev. 2010;7:CD006311.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric pes planus: A state-ofthe-art review. Pediatrics. 2016;137:e20151230.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical treatment of flexible flatfoot in children a four-year follow-up study. J Bone Joint Surg Am. 2001;83A:73-9.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of painful pediatric flatfoot with maxwell-brancheau subtalar arthroereisis implant a retrospective radiographic review. Foot Ankle Spec. 2010;3:67-72.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric flatfoot: Cause, epidemiology, assessment, and treatment. Curr Opin Pediatr. 2014;26:93-100.
- [CrossRef] [PubMed] [Google Scholar]
- Calcaneo-stop procedure in the treatment of the juvenile symptomatic flatfoot. J Foot Ankle Surg. 2013;52:444-7.
- [CrossRef] [PubMed] [Google Scholar]
- Hallux valgus correction in young patients with minimally invasive technique In: Waddell JP, ed. The role of osteotomy in the correction of congenital and acquired disorders of the skeleton. London: IntechOpen; 2012. Available from: https://www.intechopen.com/books/the-role-of-osteotomy-in-the-correction-of-congenital-and-acquired-disorders-of-the-skeleton/hallux-valgus-correction-in-young-patients-with-minimally-invasive-technique [Last accessed on 2024 Jan 26]
- [CrossRef] [Google Scholar]
- Italian translation, cultural adaptation and validation of the “American Orthopaedic Foot and Ankle Society's (AOFAS) ankle-hindfoot scale”. Acta Biomed. 2016;87:38-45.
- [Google Scholar]
- Translation, cross-cultural adaptation, reliability, and validation of the italian version of the Foot and Ankle Disability Index (FADI) Acta Biomed. 2020;91:160-6.
- [Google Scholar]
- Biodegradable device applied in flatfoot surgery: Comparative studies between clinical and technological aspects of removed screws. Mater Sci Eng C Mater Biol Appl. 2013;33:1773-82.
- [CrossRef] [PubMed] [Google Scholar]
- The surgical treatment of infantile flat foot. A new expanding endo-orthotic implant. Ital J Orthop Traumatol. 1985;11:315-22.
- [Google Scholar]
- Flexible flatfoot treatment with arthroereisis: Radiographic improvement and child health survey analysis. J Foot Ankle Surg. 2004;43:144-55.
- [CrossRef] [PubMed] [Google Scholar]
- Calcaneo-stop surgery with conical talar screw for flat-valgus foot. Capsula Eburnea. 2010;5:10-4.
- [Google Scholar]
- Application of poly-L-lactide screws in flat foot surgery: Histological and radiological aspects of bio-absorption of degradable devices. Histol Histopathol. 2012;27:485-96.
- [Google Scholar]




