
Translate this page into:
The prevalence of flatfoot among Saudi population: A systematic review
 , Afaf S. Almansoof2, Ayman H. Jawadi3MD
, Afaf S. Almansoof2, Ayman H. Jawadi3MD
*Corresponding author: Abdulmajeed S. Almansouf, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia. majeed9992008@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Almansouf AS, Alosaimi MI, Alsinan SH, Almanea RK, Almansoof AS, Jawadi AH. The prevalence of flatfoot among Saudi population: A systematic review. J Musculoskelet Surg Res 2022;6:247-55.
Abstract
Flatfoot is a foot deformity characterized by a collapsed medial arch, plantar flexion and medial rotation of the talus, eversion of the calcaneus, and forefoot abduction. The flatfoot prevalence and causes are not well known despite its correlation with multiple factors. This study aimed to systematically review all studies that estimated the flatfoot prevalence among Saudi population and list the associated factors. Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines and Joanna Briggs Institute reviewer’s manual were followed to perform this systematic review. Data collection was through several databases using terms including prevalence, Saudi, and flatfoot with their synonyms. The inclusion criteria were both adults and children’s studies that were carried out in Saudi Arabia (Saudi and non-Saudi), with the exclusion of secondary flatfoot (due to traumatic or pathological causes) studies. A total of 361 published studies before July 2021 which involved 6190 participants were reviewed, and only six studies were included in the study. The participants’ age ranged from 4.2 ± 3.6 to 37 ± 11.26 years. There was male predominance, with body mass index (BMI), age, and gender being common factors studied in the articles. Flatfoot prevalence in Saudi Arabia differed according to multiple factors as reported by different authors. This review revealed a wide range of flatfoot prevalence among the Saudi population. Most of the included studies reported that BMI, age, gender, residence, family history of flatfoot, footwear type during childhood, hypermobility, functional mobility, balance, and flexibility of the whole body had a significant impact on flatfoot prevalence.
Keywords
Flatfoot
Flattened arch
Medial arch
Pes planus
Prevalence
Saudi Arabia

INTRODUCTION
Flatfoot, also known as pes planus, is a foot deformity characterized mainly by a collapsed medial arch, plantar flexion of the talus, medial rotation of the talus, eversion of the calcaneus, and abduction of the forefoot.[1] Hindfoot valgus and forefoot supination are two of the numerous deformities that cause the term flatfoot.[2] The exact cause of flatfoot deformity is not well known despite its correlation with multiple factors, including age, gender, weight, race, and type of footwear.[3]
In children, the clinical manifestations of flatfoot extend from being flexible and painless to rigid and painful.[2] Although flexible flatfoot is considered physiological in most children, it can induce pain, which can be exacerbated by loading activities and eventually lead to early fatigue and medial foot callus.[2] In contrast, children with rigid flatfoot experience more discomfort than the flexible type, as they encounter growing pain, muscle contractures, functional limitation, and fatigue associated with joint malalignment.[2]
Flatfoot can also be acquired in adulthood. Patients may vary from being relatively asymptomatic to showing apparent symptoms.[4] Symptoms might include ankle pain, bony bumps, and a gradual onset of vague pain in the medial foot, which may worsen with activity.[4] According to two systematic reviews done in 2017 and 2018, there are no universally accepted criteria for diagnosing flatfoot.[5,6] Only three methods were recommended for further research, including the Chippaux-Smirak index, Staheli arch index, and foot posture index.[5] Therapeutic interventions are usually not required in managing flexible flatfoot since it typically resolves during the child’s first decade.[2,7] However, children with rigid flatfoot may benefit from conservative therapy or surgical interventions.[7,8] On the other hand, adults with flatfeet may use orthoses, braces, and shoe modifications as medical treatment. However, reports have shown minimal improvements in many adult cases compared to children.[9]
No systematic reviews were found studying the Saudi population based on comprehensive searching. Therefore, this study aimed to systematically review all related studies that estimated the prevalence of flatfoot among the Saudi population in both children and adults and list the associated factors.
MATERIAL AND METHODS
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and Joanna Briggs Institute (JBI) reviewer’s manual were followed to perform this systematic review of the literature on the prevalence of flatfoot among the population live Saudi Arabia (Saudi and non-Saudi).[10,11] The protocol was registered and approved by King Abdullah International Medical Research Center (KAIMRC).
Literature searching
Electronic searching for eligible peer-reviewed articles was conducted through several databases (EBESCO, EMBASE, OVID, PubMed, ISI, SCOPUS, ProQuest, and Google Scholar). In addition, reference lists of the included studies and related published systematic reviews were screened manually. Database searching terms are shown in [Table 1]. All related studies that estimated the prevalence of flatfoot in the Saudi population and fit the inclusion criteria were included in the study.
| Term | Synonymous |
|---|---|
| Prevalence | Prevalence |
| Saudi | All population in Saudi Arabia |
| Flatfoot | Pes planus, fallen arch, flat footed, pes valgus, planovalgus, low arch, flat footedness |
Selection criteria
Inclusion criteria were determined using the CoCoPop mnemonics (conditions, context, and population) used in this review.[10,12] When it came to flatfoot as a condition, the context was Saudi Arabia, and the population included both Saudis and non-Saudis living in Saudi Arabia. Therefore, this systematic review included all full-text studies diagnosed in both adults and children in Saudi Arabia and published before July 2021. There were no language restrictions. Studies examining patients with flatfoot due to secondary causes (either due to traumatic or pathological causes) were excluded from the study.
Literature quality assessment
Various important quality assessment tools have been found to evaluate prevalence surveys. In 2012, the JBI Working Group was able to develop an important rating format for assessing studies for systematic reviews of prevalence, which was well received by many authors.[12,13] Therefore, the JBI critical appraisal tools for systematic reviews checklist for prevalence studies were used for this systematic review. It included nine questions to analyze the quality of the studies. The answers to the questions were either yes, unclear, no, or not applicable. The authors had agreed to score the quality out of 18 points in total, where yes, unclear, or not equal to 2, 1, and 0, respectively. If the question was answered as not applicable, the item would be eliminated from the total.
Data extraction
The data extraction format was prearranged and validated by the authors. Data items included publication year, geographic location, the number of participants (sample size), response rate, mean age, the number of males/females, outcome (flatfoot type), data collection instrument, the cutoff score used, prevalence estimates, and associated factors. Two authors did studies’ eligibility review, quality assessment, and data extraction. They worked independently to identify, assess, and collect data from all studies. Any disagreement was resolved by a discussion with the third author.
Data analysis
Descriptive data tables were developed to explore the articles’ several extracted data. Microsoft Excel worksheet was used to calculate literature quality assessment scores and develop related graphs.
RESULTS
The searched and screened articles were arranged according to the PRISMA flowchart [Figure 1]. The review yielded 361 published studies, of which 83 duplicates were excluded, and 278 were screened based on title and abstract. Two hundred and seventy were excluded due to irrelevant population and medical conditions resulting in eight eligible studies. However, after a full-text review, no further studies were excluded from the study. After the qualitative assessment, two out of the eight studies were excluded due to invalid diagnostic instruments and inaccurate outcomes reporting. Therefore, a total of six studies were included based on the authors’ selection criteria. Manual searching did not reveal additional eligible articles.

- The of flatfoot among Saudi population Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram.
Studies main characteristics
A total of six studies, of which 6190 participants were included, published between January 2006 and March 2021, met the inclusion criteria. In addition, their quality was checked and had valuable quality scores [Figure 2].
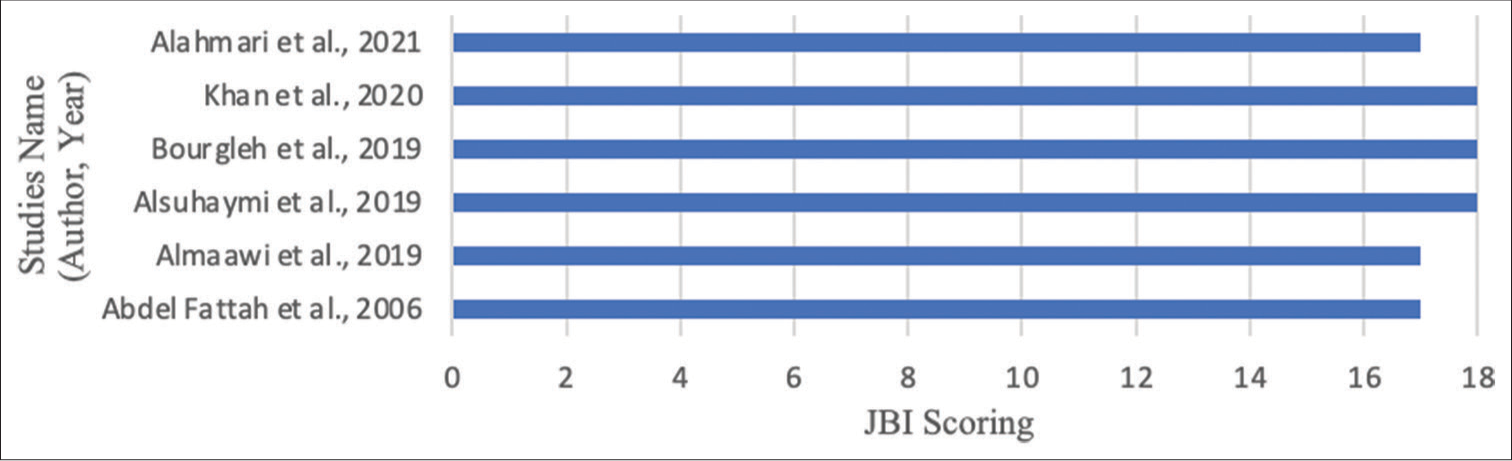
- Quality assessment scores of each included study using Joanna Briggs Institute critical appraisal tool.
All studies were conducted in Saudi Arabia from various geographical regions. The majority of the participants (5076; 82%) were from the Western region of Saudi Arabia, with only 533 (8.6%) from the central and 581 (9.4%) from the southern. Out of all the participants, only 208 (3.4%) were non-Saudis living in Saudi Arabia. The participants’ age ranged from 4 years to 40 years. Bourgleh et al. and Alsuhaymi et al. included the pediatric population with a mean age of 4.2 and 10.5, respectively. Abdel Fattah et al., Almaawi et al., Khan et al., and Alahmari et al. reported adult participants with a mean age of 19.1, 37, 21.3, and 21.7, respectively. All studies included both genders except for Abdel Fattah et al. participants, as only males were included. Females were 2328 (37.6%) and males were 3862 (62.4%) of the total number. Body mass index (BMI), age, and gender were the common factors studied. The studies main characteristics are summarized in [Table 2]. The included studies used several assessment instruments with various cutoff values to detect the presence of flatfoot [Table 3].
| Study name (author/ year) | Geographic location (region/city) | Participants population | Sample size | Age in years (Mean ± SD) | Gender, n (%) | Studied variables |
|---|---|---|---|---|---|---|
| Abdel Fattah et al., 2006 |
|
Male army, Recruitment Center at Al-Hada Armed Forces Hospital | 2100 | 19.13 ± 0.43 | Males only |
|
| Almaawi et al., 2019 |
|
Outpatients, Department of Orthopedics, College of Medicine, King Saud University | 533
|
37 ± 11.26 |
|
|
| Alsuhaymi et al., 2019 |
|
Students, various summer schools | 403 | 10.5 |
|
|
| Bourgleh et al., 2019 |
|
Outpatients, private pediatric orthopedic clinic | 2321 Participants with normal musculoskeletal variation: 764 (32.9%)
|
4.2 ± 3.6 |
|
Not reported |
| Khan et al., 2020 |
|
Students, applied medical sciences at King Abdulaziz University | 252 | 21.28 ± 1.29 |
|
|
| Alahmari et al., 2021 |
|
Outpatients, Physiotherapy Outpatient Department, King Khalid University | 581 |
|
|
|
| Study name (author/year) | Assessment instrument | Cutoff values |
|---|---|---|
| Abdel Fattah et al., 2006 | Planter footprints were applied and classified according to denis | Footprint was then classified as three grades:
|
| Almaawi et al., 2019 | Three types of footprints parameters:
|
|
| Alsuhaymi et al., 2019 |
|
Flatfoot: Staheli plantar arch index >1.15 |
| Bourgleh et al., 2019 |
|
Not reported |
| Khan et al., 2020 |
|
Foot posture was classified as:
|
| Alahmari et al., 2021 |
|
Each criterion scoring followed a scale of –2, –1, 0, +1, or+2 Scores were added for each criterion:
|
Prevalence
The literature on flatfoot prevalence in Saudi Arabia included participants in central, western, and southern regions with various age categories starting from toddlers to adults. Almaawi et al. conducted a flatfoot campaign in one of the biggest malls in Riyadh. People who were 18 years or older were asked to undergo feet examination by a podiatrist using three different footprint parameters (Clark’s Angle, Chippaux-Smirak index, and Staheli index) to define foot arch. A total of 533 male and female participants were included in this study, with a mean age of 37 ± 11.26 years, of which 417 (78.2%) were Saudis and 116 (21.8%) nonSaudis. Based on Clark’s angle index, 221 (41.5%) right feet and 216 (40.5%) left feet had flattened arches. Similarly, 72 (13.5%) right feet and 67 (12.6%) left feet had flat arches based on the Chippaux-Smirak index, and 51 (9.6%) right feet and 45 (8.4%) left feet based on the Staheli index. According to Abdel Fattah et al., among 2100 Saudi army recruits with an age group of 18–21 years in Taif, 104 (5%) participants were diagnosed with flatfeet. Khan et al. reported an estimated prevalence of 64 (25%) cases of flatfeet among 252 medical students using foot posture index-6 in King Abdulaziz University, Jeddah. They concluded that females had a higher flatfoot prevalence (81.75%) than males (18.75%). Likewise, Alahmari et al. reported that females (21.0%) had a higher incidence of pronation than males (16.8%). Out of the 581 patients, 110 (18.9%) had pronated and 41 (7.1%) had hyperpronated flatfeet using the FBI score at the outpatient physiotherapy department in King Khalid University, Abha. Alsuhaymi et al. conducted a study in Almadinah Almunawwarah, which showed that out of 403 school-aged children at multiple summer schools with ages ranging 7–14 years, flatfoot was witnessed in 119 (29.5%) students. Flexible flatfoot was found in 96.6% and rigid flatfoot was found in 3.4%, with the 7–8 age group being the highest. In Bourgleh et al., 2321 patients <12 years old who visited a private pediatric orthopedic clinic had normal musculoskeletal variation detected in 764 patients (32.9%), out of which 672 (88%) were Saudis, and 92 (12%) were nonSaudis. Flexible flatfoot was observed in 309 (41.9%) of these 764 patients.
Factors associated with flatfoot
All articles studied the relationship between BMI and flatfoot except for Bourgleh’s et al. study. Flatfoot was significantly higher among all participants with high BMI (P < 0.05), excluding Alsuhaymi et al., where no significant correlation was found (P = 0.636). Out of six articles, five studied the relationship between age and flatfoot. Age was found to be a significant factor (P < 0.05) in the development of flatfoot in four studies; while Khan et al. reported no significance (P = 0.08). Bourgleh et al. (P = 0.73) and Alsuhaymi et al. (P = 0.66) found no significant association between gender and the occurrence of flatfoot. On the other hand, gender was significantly associated with flatfoot in Almaawi et al., using Clark’s angle (P = 0.001) and in Khan et al., using FPI-6 (P = 0.03). Other predictors of flatfoot, such as residence, family history of flatfoot, and type of footwear during childhood, were reported to be significant in Abdel Fattah et al. study. Hypermobility, functional mobility, and balance were all significant variables mentioned in Alahmari’s et al. article. Likewise, Khan et al. found that ligament laxity of the whole body was associated with flatfoot. Other factors are listed in [Table 4].
| Study Name (Author/ Year) | Overall Prevalence Estimates n (%) | Significant Associated Factors (P-Value < 0.05) | Non-Significant Associated Factors |
|---|---|---|---|
| 1. Abdel Fattah et al., 2006 |
|
|
|
| 2. Almaawi et al., 2019 |
|
|
|
| 3. Alsuhaymi et al., 2019 |
|
|
|
| 4. Bourgleh et al., 2019 |
|
|
|
| 5. Khan et al., 2020 |
|
|
|
| 6. Alahmari et al., 2021 |
|
|
|
DISCUSSION
This is the first systematic review that revealed a wide range of flatfoot prevalence among the Saudi population. The prevalence of flatfoot reported by different authors worldwide had great variations. The fact that the authors used different methods could explain these differences. Among adults, globally, a cross-sectional study conducted in Spain estimated the prevalence of flatfoot as 26.62% in 835 patients over the age of 40, with a higher incidence in older patients.[1] Japan which showed nearly identical results to Spain’s exhibited a prevalence of 26.5%, with 340 (242 women and 98 men) participants aged 60 and above who were neither hospitalized nor disabled in their regular activities.[14] In Saudi Arabia, Almaawi et al. used three different footprint parameters: Clark’s angle, Chippaux-Smirak index, and Staheli index, to define foot arch.[15] As shown in [Table 4], there are wide variations between the results of each parameter in the study. However, the Chippaux-Smirak and Staheli indices exhibited a significant concordance in diagnosing flatfoot with kappa value >0.8 and P < 0.05.[15] In India, a cross-sectional study was done in 2017 with 500 healthy Indian participants (250 males and 250 females) aged 18–21 years who reported a flatfoot prevalence of 13.6% (12.8% of males and 14.4% of females).[16] Abdel-Fattah et al. reported a flatfoot prevalence of 5% in 2100 male army recruits in Taif, Saudi Arabia, in a similar age group.[17] Worth noting, there may be an inherent bias as known patients with flatfoot would not apply to the military. In addition, Khan et al. concluded that among 252 participants aged 18–25 years, 64 (25%) of the cases had flatfoot using FPI-6 in Jeddah, Saudi Arabia.[18] Noticeably, females showed a higher flatfoot prevalence (81.75%) than males (18.75%).[18] According to Alahmmari et al. article, out of 581 individuals, 110 (18.9%) pronated and 41 (7.1%) hyperpronated feet were found; similar to the previous literature, females (21.0%) had greater pronation rates than males (16.8%).[19] Likewise, in Boston, the United States, a study reported that the incidence of flatfoot in females is higher by 3% than in males.[20]
In children, flatfoot has been reported as one of the most common foot disorders internationally.[3] A study in Austria that included 835 children aged 3–6 years reported that 44% of them had flexible flatfoot, and males had a greater tendency.[21] In Taiwan, a study with 2083 children aged 7–12 years estimated that 59% had flatfoot.[22] Similarly to Austria, flatfoot is twice as common in males as in females.[21,22] A cross-sectional study was conducted in Islamabad on 714 students aged 6–10 years.[23] It showed that the prevalence of flatfoot was 14.8% and more common in males as in the Taiwanese and Austrian studies.[21-23] In Jeddah, Bourgleh’s et al. study aimed to determine the normal musculoskeletal variations in 2321 children (88% Saudis) who were <12 years of age, and reported that 309 (41.9%) had flatfeet.[24] In Alsuhaymi et al. article, the 7–8-year-old group had the highest rate of flatfoot out of 403 school-aged children from various summer schools in Almadinah Almunawwarah, similar to the Taiwanese study.[25]
Multiple studies examined the association between gender and the presence of flatfoot.[15,18,26] In Nigeria, a study revealed a significant association between flatfoot and gender, in which flatfoot was 3 times more prevalent in females than males.[26] Similarly, two studies, Almaawi et al. and Khan et al. done in Saudi Arabia, have found that females are more prone to the development of flatfoot than males.[15,18] Khan’s et al. article showed that wearing high heels among young adult females were a possible risk factor for the increased prevalence of flatfoot in females using the center of pressure excursion index.[18] When comparing genders in Almaawi et al. study, females had a higher prevalence of foot pronation using Clark’s angle, while Chippaux-Smirak index and Staheli index showed higher prevalence in males.[15] Contradictory to our studies, a study in the United States, Texas, concluded that flatfoot deformity was strongly associated with the male gender.[27] This is thought to be due to the fact that the majority of participants were from the veteran population.[27] Globally, the prevalence of flatfoot varies with age.[27,28] Age was thought to be the primary predictive factor for flatfoot in a study done in Congo, Central Africa, where the youngest age group, 3–4 years, had a higher proportion of a descending medial arch.[28] Consistent with the previous article, Bourgleh et al. examined the prevalence of flatfoot among children aged 12 years or younger, and concluded that the highest incidence age at presentation was between 3 and 4 years.[24] Likewise, Alsuhaymi et al. studied children aged 7–14 years old and found that age was significantly associated with flatfoot.[25] Among other age groups, the 7–8 years group was rated the highest in prevalence.[25] Alahmari et al. investigated the significance of age in younger adults aged 18–25, while Almaawi et al. participants were older adults aged more than 45 years.[15,19] Both found a significant relationship using different foot posture measurements.[15,19] BMI is strongly related to the development of foot deformities.[29] In one Indian study, the distribution of flatfoot was found to be most prevalent in individuals categorized as morbidly obese with a BMI of 40 or more.[29] Thus, the study concluded a directly proportional relationship between BMI and flat-arched foot.[29] Similar results also illustrated a significant correlation between high BMI and flatfoot, which multiple authors have concluded in various countries.[15,17,18,26] This relationship is thought to be due to pressure over the foot arch caused by fat deposition, which leads to extreme mechanical loading while walking.[26] Equivalent to the previous studies, in Saudi Arabia, four articles showed a significant correlation between the flat-arched foot and an increased BMI.[15,17-19] Inconsistent with the aforementioned studies, Alsuhaymi et al. article showed no significant relationship.[25] Notably, a slight increase in weight could crucially affect the plantar fascia, while a slight weight reduction can drastically decrease plantar loading.[15] One study showed that losing more than 2 kg could ease foot pain and control functional limitations.[15]
The literature regarding the use of footwear during early childhood and its association with the occurrence of flatfoot is consistent both globally and locally.[17,30] In India, a survey that included 2300 children stated that children who wore shoes had a significantly higher prevalence of flatfoot than barefooted children.[30] Likewise, Abdel Fattah et al. reported that the type of footwear used during early childhood was a key factor in diagnosing flatfoot later in life.[17] This establishment was done by studying both children who wore shoes and those who were barefooted.[17] To the best of our knowledge, only Abdel Fattah et al. examined the relationship between flatfoot and family history, which was a highly significant risk factor.[17] Other multiple significant factors associated with flatfoot, such as hypermobility, functional mobility, the flexibility of the whole body, and balance, have been reported in several articles.[18,19]
Limitations
Significant results heterogeneity found in the included studies suggested associations with multiple reasons, including various studies’ methods and diagnostic instruments.
CONCLUSION
Most of the included studies reported that BMI, age, gender, residence, family history of flatfoot, type of footwear during childhood, hypermobility, functional mobility, balance, and ligaments laxity of the whole body had a significant impact on the prevalence of flatfeet.
RECOMMENDATIONS
High-quality multicenter epidemiological studies are required. Adopting standardized diagnostic instruments are essential to enable and identify the existence of flatfoot accurately and allow valid and generalizable recommendations.
ACKNOWLEDGMENT
The authors would like to thank Mr. Mohammed Al Sawadi, the Medical Library Technician, for his valuable search support.
AUTHORS’ CONTRIBUTIONS
ASA: Reviewer of the study selection, reviewer of the quality assessment, and manuscript writing. MIA: Reviewers of the study selection, reviewer of the data extraction, and manuscript writing. SHA: Reviewer of the study quality assessment and manuscript writing. RKA: Reviewer of data extraction, reviewer of the study selections, and manuscript writing. ASA: Reviewer of the study quality assessment, data extraction, and manuscript writing. AHJ: Principal investigator and supervisor. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
ETHICAL APPROVAL
Research ethics board approval was gained before starting any study procedure. This review’s ethical approval was obtained from the KAIMRC in Saudi Arabia (IRB Ethical approval no: RYD-21-419812-117792) (IRB Ethical approval date: August 25, 2021).
DECLARATION OF PATIENT CONSENT
Patients' consent was not required as there are no patients in this review.
FINANCIAL SUPPORT AND SPONSORSHIP
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
CONFLICTS OF INTEREST
There are no conflicting relationships or activities.
References
- Flat foot in a random population and its impact on quality of life and functionality. J Clin Diagn Res. 2017;11:LC22-7.
- [Google Scholar]
- Flexible flatfoot in children and adolescents. J Child Orthop. 2010;4:107-21.
- [CrossRef] [PubMed] [Google Scholar]
- Flatfoot prevalence and foot dimensions of 5-to 13-year-old children in Taiwan. Foot Ankle Int. 2009;30:326-32.
- [CrossRef] [PubMed] [Google Scholar]
- Tibialis posterior tendon rupture. Clin Orthop Relat Res. 1983;177:140-7.
- [CrossRef] [Google Scholar]
- The effectiveness of non-surgical intervention (foot orthoses) for pediatric flexible pes planus: A systematic review: Update. PLoS One. 2018;13:e0193060.
- [CrossRef] [PubMed] [Google Scholar]
- The typically developing pediatric foot: How flat should it be? A systematic review. J Foot Ankle Res. 2017;10:37.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric flatfoot: Cause, epidemiology, assessment, and treatment. Curr Opin Pediatr. 2014;26:93-100.
- [CrossRef] [PubMed] [Google Scholar]
- The diagnosis and management of common childhood orthopedic disorders. Curr Probl Pediatr Adolesc Health Care. 2011;41:2-8.
- [CrossRef] [PubMed] [Google Scholar]
- Current concepts and correction in the valgus foot. Clin Orthop Relat Res. 1970;70:43-55.
- [CrossRef] [Google Scholar]
- Systematic reviews of prevalence and incidence In: Joanna Briggs Institute Reviewer's Manual. Adelaide, South Australia: The Joanna Briggs Institute; 2017. p. :5-1.
- [Google Scholar]
- Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009;6:e1000097.
- [CrossRef] [PubMed] [Google Scholar]
- The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag. 2014;3:123-8.
- [CrossRef] [PubMed] [Google Scholar]
- Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Healthc. 2015;13:147-53.
- [CrossRef] [PubMed] [Google Scholar]
- Association of flatfoot with pain, fatigue and obesity in Japanese over sixties. Nihon Koshu Eisei Zasshi. 2003;50:988-98.
- [Google Scholar]
- Flatfoot prevalence in Riyadh city Saudi Arabia and its association with obesity, using three footprint indices; Clark's angle, chippaux-smirak index, and staheli index. Orthop Rheumatol Open Access J. 2019;15:52-8.
- [CrossRef] [Google Scholar]
- Prevalence of flexible flat foot in adults: A cross-sectional study. J Clin Diagn Res. 2017;11:AC17-20.
- [CrossRef] [PubMed] [Google Scholar]
- Flat foot among Saudi Arabian army recruits: Prevalence and risk factors. East Mediterr Health J. 2006;12:211-7.
- [Google Scholar]
- Factors affecting foot posture in young adults: A cross sectional study. J Musculoskelet Neuronal Interact. 2020;20:216-22.
- [Google Scholar]
- Foot posture index reference values among young adults in Saudi Arabia and their association with anthropometric determinants, balance, functional mobility, and hypermobility. BioMed Res Int. 2021;2021:1-10.
- [CrossRef] [PubMed] [Google Scholar]
- Footprint analysis of flatfoot in preschool-aged children. Eur J Pediatr. 2011;170:611-7.
- [CrossRef] [Google Scholar]
- Prevalence of flat foot in preschool-aged children. Pediatrics. 2006;118:634-9.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of flexible flatfoot in Taiwanese school-aged children in relation to obesity, gender, and age. Eur J Pediatr. 2010;169:447-52.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of the flat foot in 6-10 years old school going children. Rawal Med J. 2013;38:385-7.
- [Google Scholar]
- Prevalence of musculoskeletal normal variations of the lower limbs in pediatric orthopedic clinic. Saudi Med J. 2019;40:930-5.
- [CrossRef] [PubMed] [Google Scholar]
- Flatfoot among school-age children in Almadinah Almunawwarah: Prevalence and risk factors. J Musculoskelet Surg Res. 2019;3:204-8.
- [CrossRef] [Google Scholar]
- Adult flat foot and its associated factors: A survey among road traffic officials. Nov Tech Arthritis Bone Res. 2019;3:1-3.
- [Google Scholar]
- Characteristics of adult flatfoot in the United States. J Foot Ankle Surg. 2010;49:363-8.
- [CrossRef] [PubMed] [Google Scholar]
- The development in footprint morphology in 1851 Congolese children from urban and rural areas, and the relationship between this and wearing shoes. J Pediatr Orthop B. 2003;12:141-6.
- [CrossRef] [Google Scholar]
- A study on relationship between BMI and prevalence of flat foot among the adults using foot print parameters. Int J Adv Res. 2016;4:1428-31.
- [CrossRef] [Google Scholar]
- The influence of footwear on the prevalence of flat foot. A survey of 2300 children. J Bone Joint Surg Br. 1992;74:525-7.
- [CrossRef] [PubMed] [Google Scholar]




