
Translate this page into:
Traumatic injuries in children and youth from Southern Brazil: A cross-sectional study
*Corresponding author: Jamil F. Soni, School of Medicine, Pontifical Catholic University of Paraná, Curitiba, Paraná, Brazil. jamilfsoni@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Soni JF, Sandrin ND, Franco de Oliveira PR, Possamai AF, Ferreira AL, Garbers LA, et al. Traumatic injuries in children and youth from Southern Brazil: A cross-sectional study. J Musculoskelet Surg Res 2022;6:25-31
Abstract
Objectives:
The objective of the study was to identify the prevalence of firearm injuries (FI) and bladed weapon injuries (BWIs) in underage people and their respective outcomes.
Methods:
Using a retrospective observational design, data were recorded on patients who met the inclusion criteria receiving care in a public hospital between June 30, 2015, and June 30, 2018.
Results:
Ninety-one medical records were found, 76.9% of patients were males and 23.1% were females. Most injuries were caused by firearms (76%) and the remainder by bladed weapons (24%). The majority of patients were 12–18 years old (92.3%), while 7.7% were 6–12 years old. Male participants were the ones who most needed medical care (77%). Male adolescents in the older age group with injury-associated fractures (P = 0.015 and P = 0.032) accounted for the most common association in the sample, demonstrating greater susceptibility to fractures in these groups. Analysis of detailed location proved that BWIs BWIs were the leading cause of injuries to soft abdominal organs (P = 0.011).
Conclusion:
The occurrence of FI and BWIs in the pediatric population is significant and can imply death and tragic sequelae. Emergency services need to be prepared to provide care to these victims, particularly males and the 12–18 age range, as these are the most affected groups. Further studies should be conducted on this theme to gain a greater and better understanding of the etiology and repercussions of this type of injury in the lives of young patients.
Keywords
Adolescent
Bladed weapon
Child
Firearms
Fracture
Gun violence
Injury

INTRODUCTION
Healthcare for children and adolescent victims of firearm injuries (FI) and bladed weapon injuries (BWI) more often requires more surgical interventions and longer rehabilitation time, as well accounting for a relative increase in mortality rates.[1] Etiologically, these types of injuries reflect the somatization of issues that are both behavioral and social. On the psycho-behavioral level, curiosity, which is inherent to children and adolescents, is indicated as one of the factors resulting in this age range suffering this type of trauma, especially in cases where it is accidental. Moreover, adolescents are also exposed to alcohol and drug abuse, which is directly and indirectly, related to FI.[2]
According to the adolescent homicide rate (which estimates the risk of adolescents–12−18 years old–losing their lives due to violence), published in 2010, 781 deaths are expected between 2015 and 2021 in the city of Curitiba alone. Indicated by that study as being the most dramatic cities in Southern Brazil in relation to underage homicide victims, the Greater Curitiba region cities of Pinhais and Almirante Tamandaré exceed the rate of six adolescent homicide victims per 1000 adolescents.[3] Understanding the profile of the victims is important, as more than 92% of youth homicides affect males.[4]
Studies demonstrate that a 1% increase in firearm proliferation culminates in a rise of approximately 2% in homicide rates.[5] On average, children and adolescents account for 20.7% of total firearm victims in Brazil, meaning that one in five Brazilians murdered by gunshots in 2015 were under 19 years old.[6]
In turn, as bladed weapons are an easy-to-access violence and injury tool, they play an outstanding role in urban violence rates. According to a study conducted in the North Paraná University Hospital in Londrina in 2007, 45 people received emergency care as victims of BWI.[4] This fact reiterates the importance of studying this type of injury present in the state of Paraná. In 2006, 74.4% of homicides in Brazil were due to FI, while BWI caused 16.1%. These last data represent an increase of 2.3% of homicides caused by BWI when compared to the year 2000. Therefore, it can be inferred that increased use of bladed weapons can be attributed to easier access and less control when compared to firearms, as well as to population growth, civil violence and passional crimes.[4]
In addition, emergency services are important because they are the entry point for cases of violence. Physical injuries presented to emergency services manifest themselves profusely and involve, above all, injuries to the head, neck, and extremities. They have diverse forms such as contusions, lacerations, severe traumatic brain injuries, and fractures.[7] Adolescents are most frequently involved in more serious situations, with higher risk injuries caused using firearms. Injuries caused by physical aggression or assault are generally milder and rarely need hospitalization. Given the nature of this emergency care, a need can be seen to discuss greater attention to the health of children and adolescents who suffer violent traumas, thus increasing the importance of this question on the psychosocial level.
Psychological effects arising from urban violence can be identified at initial care in emergency services and persist after the traumatic experience has ended. Consequently, the child or adolescent remains with symptoms of acute stress, fear, terror or helplessness, along with more complex disorders in the initial stage of trauma, increasing the possibility of future psychological changes.[8]
In general, analysis of this circumstance reveals issues of great social importance, highlighting problems that involve two primordial public policy areas: Health and security. Based on the analysis of these data, it can be perceived that many children and adolescents live in environments with a high risk of violence, whereby the fundamental right to security is neglected. The argument here also relates to exploring the seriousness of the correlation between health and public security. The scenario highlights the urgency of studying in-depth the phenomenon of child and youth homicides.
Finally, the main objective of this study is to identify the prevalence of specific injuries and their correlations with age and trauma mechanism in a tertiary emergency hospital in the city of Curitiba.
MATERIALS AND METHODS
This is a retrospective observational study that observed firearm and BWIs s in a general hospital by examining medical records over 3 years, from June 30, 2015, to June 30, 2018. The study included patients aged 18 years or under who had suffered firearm or BWIs s referred to the Hospital do Trabalhador, a trauma reference center with more than 200 hospital beds, providing care exclusively for Brazilian National Health patients System. Patients with incomplete medical records were excluded from the study.
The following information was retrieved and recorded for each case: Gender; type of injury (FI/BWI); and patient’s age at the time of trauma, which was divided into age groups as defined by the Child and Adolescent Statute,[9] where age group 1 was 0–6 years, age group 2 was 6–12 years, and age group three was 12-18 years; trauma mechanism (location; whether there were fracture(s) and type of fracture(s)), type of case management (conservative, when sutures or plaster and orthopedic splints were applied in the emergency service; general surgery management; orthopedic management; and both managements or whether the patient left the hospital before being discharged), treatment given (individualized for each case), and length of inpatient stay and outcome (discharge, complications, or death).
The data were stored on an electronic spreadsheet (Microsoft Excel 2007®. Redmond, WA, USA). Length of inpatient stay (days) was expressed as medians, minimum values, and maximum values. The results of the categorical variables were described according to frequencies and percentages. Fisher’s exact test was used to assess for an association between two categorical variables. Comparison between types of case management in relation to the length of inpatient stay was made using the Kruskal–Wallis non-parametric test. P < 0.05 indicated statistical significance. The data were analyzed using the IBM SPSS Statistics computer program, (v.20.0, Armonk, NY; IBM Corp).
The following variables were compared: Gender versus FI/ BWI; gender versus location (single/associated); gender versus associated fracture (presence/absence); age group versus FI/BWI; age group versus topography (single/ associated); age group versus associated fracture (presence/ absence); length of inpatient stay (0/≥1 day) versus case management; detailed associated fracture versus FI/BWI; detailed associated fracture versus gender; detailed associated fracture versus age group; detailed topography versus FI/ BWI; and detailed topography versus gender.
RESULTS
Among 120 medical records examined for eligibility, 29 were excluded because of incomplete medical charts. Thus, there were 91 medical records included in the study and analyzed. On those, FIs were more prevalent than BWIs, as 69 patients (76%) were victims of FIs, while 22 (24%) were victims of BWIs. In the period studied, no children in the first age group (0–6 years) received care. There were seven patients in the second (6–12 years) age group (7.7%) and the remainder fell into the third (12–18 years) age group (92.3%). The male gender was predominant and accounted for 70 patients (77%), whereas females accounted for 21 patients (23%). Notwithstanding, FIs were more frequent in both genders.
Most injuries in the study were single-location injuries, occurring in 59 cases, 49 of which were caused by firearms. Around two-thirds (62 victims; 68%) of the injuries had no associated fractures [Table 1].
| Variable | Classification | n | Percentage |
|---|---|---|---|
| Gender | Female | 21 | 23.1 |
| Male | 70 | 76.9 | |
| FI/BWIs | FI | 69 | 75.8 |
| BWIs | 22 | 24.2 | |
| Age group (ECA) | 2 (from 6 to 12 years) | 7 | 7.7 |
| 3 (from 12 to 18 years) | 84 | 92.3 | |
| Type of management | Conservative | 52 | 57.1 |
| General surgery | 25 | 27.5 | |
| Orthopedic surgery | 11 | 12.1 | |
| Geneneral+Orthopedics | 2 | 2.2 | |
| Left hospital before treatment | 1 | 1.1 | |
| Length of hospitalization* | 0 | 39 | 42.9 |
| (Days) | ≥1 day | 52 | 57.1 |
| Detailed outcome | Hospital discharge without sequelae | 59 | 64.8 |
| Hospital discharge with total sequelae | 25 | 27.5 | |
| Hospital discharge with parcial sequelae | 1 | 1.1 | |
| Death with organ donation | 6 | 6.6 | |
| Death | No | 85 | 93.4 |
| Yes | 6 | 6.6 | |
| Sequelae | Yes | 32 | 35.2 |
| No | 59 | 64.8 |
ECA: Abbreviation, in Portuguese, to Child and Adolescent Statute. *The medium length of hospitalization was 2 days (minimum 0, maximum 44 days), FI/BWIs: Firearm injuries/bladed weapon injuries
Concerning case management, 52 (57.1%) patients received conservative treatment, 25 (27.5%) underwent general surgery procedures, 11 (12.1%) were submitted to orthopedic surgery, and two (2.2%) underwent both kinds of surgery; one patient (1.1%) left the hospital before receiving treatment. All patients who received surgical treatment remained in the hospital for some time equal to or >1 day. This length of time was greater than it was for those submitted to conservative treatment (P = 0.001).
Of the 91 patients analyzed, 6 (6.6%) died while they were still in hospital, 59 (64.8%) were discharged with no sequelae while 32 (35.2%) patients left the hospital with sequelae. In the present study, any permanent anatomical and/or functional change that was caused by the accident in question (FI or BWI) was considered a sequela. A relationship was found between gender and associated fracture (P = 0.015), where the presence of associated fracture was predominant in males (38.6%) compared to females (9.5%). However, no significant difference was found when comparing gender with single/associated location (P = 0.605) and firearm/ bladed weapon as the instrument causing injury (P = 0.772).
We found a statistical relationship between victim age group and occurrence of fractures (P = 0.032), whereby the presence of fractures was predominant in the second age group (71.4%) when compared to those in the third age group (28.6%). The p-values for the other variables were 0.189 and 0.693, respectively [Figure 1].
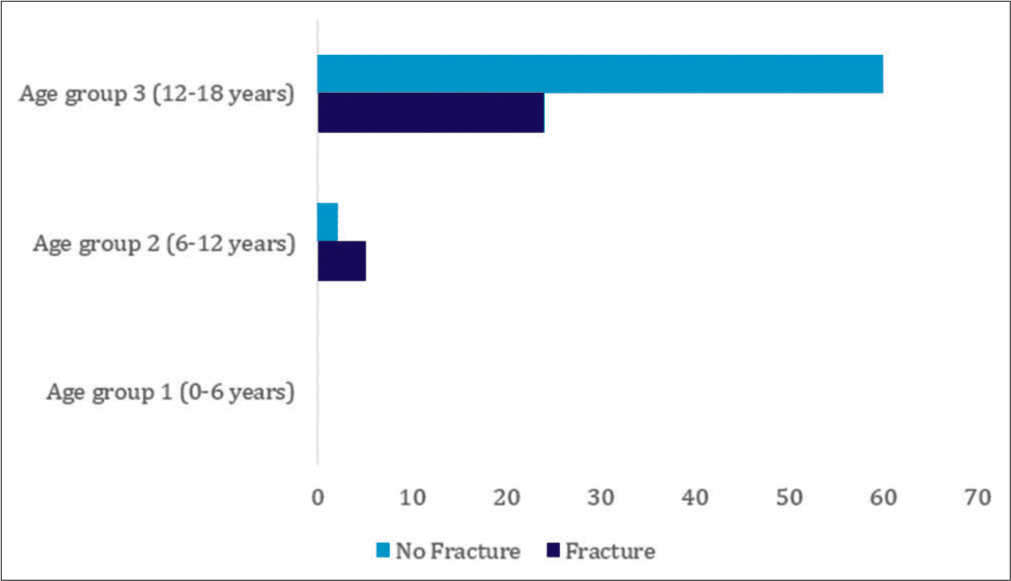
- Demonstration of the relationship in percentages between the groups separated by age group (ECA) and associated fractures (presence/absence).
Analysis of the detailed location of injuries in relation to FI/BWI was only tested for the most affected regions [Table 2], we obtained significant relationship with soft abdominal masses (not specified) injuries (P = 0.011). This revealed occurrence of a statistical relationship between soft abdominal organ injury and the instrument that caused the injury, whereby the majority of the five patients with this kind of injury were victims of BWI (18.2%). Detailed injury location was also tested in relation to the victim’s gender [Table 2]. Once again, only the main injury locations were analyzed, but no significant difference was found between the variables.
| Location | n | % |
|---|---|---|
| Adrenal gland | 1 | 1.1 |
| Arterial system abdomen | 1 | 1.1 |
| Arterial system cranium | 1 | 1.1 |
| Bladder | 1 | 1.1 |
| Central nervous system | 6 | 6.6 |
| Cervical spine | 2 | 2.2 |
| Ear | 1 | 1.1 |
| Esophagus | 1 | 1.1 |
| Eye orbit region | 1 | 1.1 |
| Hip | 2 | 2.2 |
| Left arm | 8 | 8.9 |
| Left foot | 6 | 6.6 |
| Left forearm | 2 | 2.2 |
| Left hand | 4 | 4.4 |
| Left kidney | 1 | 1.1 |
| Left leg | 1 | 1.1 |
| Left lung | 9 | 9.9 |
| Left thigh | 9 | 9.9 |
| Left wrist | 1 | 1.1 |
| Liver | 4 | 4.4 |
| Lumbar spine | 3 | 3.3 |
| Mandible | 2 | 2.2 |
| Maxilla | 4 | 4.4 |
| Mouth | 1 | 1.1 |
| Neck venous system | 2 | 2.2 |
| Ovary | 1 | 1.1 |
| Pelvis | 2 | 2.2 |
| Pharynx | 1 | 1.1 |
| Rectum | 1 | 1.1 |
| Right arm | 8 | 8.8 |
| Right foot | 1 | 1.1 |
| Right forearm | 4 | 4.4 |
| Right hand | 3 | 3.3 |
| Right kidney | 2 | 2.2 |
| Right leg | 4 | 4.4 |
| Right lung | 3 | 3.3 |
| Right shoulder | 4 | 4.4 |
| Right thigh | 12 | 13.3 |
| Scalp | 2 | 2.2 |
| Sigmoid colon | 1 | 1.1 |
| Small intestine | 6 | 6.6 |
| Soft abdominal organ (unspecified) | 5 | 5.5 |
| Soft thorax organ | 2 | 2.2 |
| Stomach | 3 | 3.3 |
| Transverse colon | 2 | 2.2 |
| Urethra | 1 | 1.1 |
The total number of injuries was considered, regardless of whether the patient had single or multiple injuries. LOCATIONS with n=0 are not shown in the table. FI/BWIs: Firearm injuries/bladed weapon injuries
Concerning the expanded sample of the group with fractures associated with injuries [Table 3], we compared patients without fractures with FI/BWI (P < 0.001), gender (P = 0.015), and age group (P = 0.032). This revealed that of the 62 patients who did not have associated fractures, 40 were FI victims (58%) and 22 were BWI victims (100%), thus demonstrating that none of the BWI victims had associated fractures. Moreover, among these patients without associated fractures, the females (90.5%) predominated over males (61.4%); and the third age group (71.4%) predominated over the second (28.6%).
| n | % | |
|---|---|---|
| No fractures | 62 | 68.1 |
| Cervical spine | 2 | 2.2 |
| Cranial bones | 2 | 2.2 |
| Humerus | 1 | 1.1 |
| Left femur | 4 | 4.4 |
| Left foot | 3 | 3.3 |
| Left forearm | 1 | 1.1 |
| Left hand | 1 | 1.1 |
| Left humerus | 2 | 2.2 |
| Left wrist | 1 | 1.1 |
| Lumbar spine | 2 | 2.2 |
| Mandible | 3 | 3.3 |
| Maxilla | 3 | 3.3 |
| Pelvis | 2 | 2.2 |
| Right femur | 1 | 1.1 |
| Right forearm | 3 | 3.3 |
| Right hand | 1 | 1.1 |
| Right humerus | 3 | 3.3 |
| Right tibia | 1 | 1.1 |
| Thoracic spine | 1 | 1.1 |
The total number of associated fracture injuries was considered, regardless of whether the patient had single or multiple fracture locations. FI/BWIs: Firearm injuries/bladed weapon injuries
DISCUSSION
As published by the Atlas da Violência in 2017,[6] 92% of FI affected males; in our study, 74.3% of FI victims were males. Atlas of Violence is a portal that gathers, organizes, and makes available information about violence in Brazil, as well as gathers Institute for Applied Economic Research publications on violence and public safety. Although the Atlas of Violence percentage is not exclusive to the age group in our study, hence the difference, this indicated that our study followed the national trend of male propensity to this type of injury.
The third age group and the male gender were predominant in our study. This is in agreement with the national trend, whereby most firearm victims are young males involved in crime.[10] Association of fractures with the study’s second age group (6–12 years) is similar to that found by a study from the United States,[11] which defined the peak in fractures among pediatric patients in the 9–14 age group. This relationship probably occurs both because of exposure to violence (greater than in the first age group) and also because of bone system immaturity, which is more fragile when compared to the third age group (12–18 years), when growth cartilage closure occurs and marks skeleton system maturity.
The predominance of trauma caused by firearms compared to bladed weapons may be related to the fact that the state of Paraná, (where the study was conducted) is the Brazilian state with the second-highest number of legal weapons per 100,000 inhabitants.[10] This means that a comparative analysis with other states and estimates of illegal weapons would be necessary to establish a more precise association.
When analyzing the location of FIs and BWIs, we found that BWIs were the leading cause of injuries to soft abdominal organs, accounting for 18.2% of the sample. In addition to suggesting a trauma mechanism common to violence caused by bladed weapons, this demonstrates the importance of training and case management involving soft-tissue trauma related to these instruments.
The expanded sample of the anatomic regions most affected by FI/BWI, according to total injury incidence, reveals that the most affected regions were the upper limbs (n = 31, 22%), the lower limbs (n = 26, 18%), and the abdomen (n = 23, 16%) [Table 2]. This is in keeping with previous studies,[4,7] which indicated multiple upper body organs as the part of the body most affected by firearms and bladed weapons. In addition, most patients in our study, left the hospital without sequelae, which is in agreement with a similar study,[4] as the majority of injuries did not cause permanent disability, not considering death.
In view of the worsening of domestic violence against children and adolescents resulting from quarantine put in place as a form of combating the COVID-19 pandemic,[12] the possibility exists of FIs and BWIs incidence increasing significantly. As such, the results obtained by this study can assist in the analysis of possible most affected anatomic regions, most exposed age range and gender, as well as estimating, based on this data, necessary length of inpatient stay and the possibility of surgical intervention being necessary, for example.
The limitations of this study include the fact that when the data were collected, many medical records were incomplete, and this was an exclusion criterion. Moreover, the difference in medical descriptor-dependent details between one set of medical records and another was a factor that restricted the number of variables analyzed and subsequent comparison between them. When the data were collected, it was impossible to characterize injuries as intentional or unintentional because this information was missing on the medical records. When analyzing each variable individually, the fact of each patient having received individualized treatment, based on location and degree of harm, as well the presence or otherwise of associated fracture(s), made it impossible to compare this variable with the other variables, as well as restricting its analysis on a case-by-case basis. When analyzing associated fractures in detail, it was impossible to compare each fracture with the gender, FI/ BWI and age group variables due to the small number of cases for each location where injury-associated fractures occurred.
The broad database enabled diverse statistically significant correlations to be established, as shown above, even despite the specificity of the theme and the study’s inclusion criteria and also despite the fact that data collection was restricted to just one, out of three, of the specialized trauma centers serving the city of Curitiba and the Greater Curitiba region. By itself, this demonstrates the relevant incidence and, therefore, the importance of a detailed analysis of these types of injury in the population in question.
CONCLUSION
The number of FI and BWI in the pediatric population cannot be underrated, especially among males. We found a significant prevalence of fractures associated with these injuries, as well as among the 12–18 -year-old population, which was predominant in this study.
RECOMMENDATIONS
As a measure for raising the general population’s awareness, we stress the need for educational and preventive actions about the use of firearms and bladed weapons. Schools can be considered to be essential as a means of preventing criminality, given that they reduce young people’s exposure to violence. However, school infrastructure and communication with the community need to be improved, given that violence in the outside environment is increasingly reproduced inside educational environments.
Based on this study, we noted that further studies should be conducted on this theme in order to gain a greater and better understanding of the etiology and repercussions of this type of injury in the lives of patients, both physically as in this study, and also psychologically in the short term and, if possible, in the long term.
AUTHORS’ CONTRIBUTIONS
JFS contributed with the concepts, design, definition of intellectual content, literature search, data acquisition, data analysis, statistical analysis, manuscript editing and review, and manuscript preparation. NMS, PRFO, and AFP contributed with design, literature search, data acquisition, data analysis, manuscript preparation, manuscript editing, and review. ALCF contributed with design, literature search, data analysis, manuscript preparation. LAFG contributed with data acquisition, data analysis, and manuscript editing and review. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
ETHICAL APPROVAL
This study was reviewed and approved on October 10, 2018, by the local Committee in Ethics in Research (Comitê de Ética da Pontifícia Universidade Católica do Paraná, Curitiba, PR, Brazil, protocol number 2.955.860). The research study project protocol was submitted to the Hospital do Trabalhador Human Research Ethics Committee in CuritibaPR, as per the Certificate of Submission for Ethical Appraisal: 95985218.8.0000.0020.
Declaration of patient consent
The authors reinforce that there was no contact between researchers and participants. The analysis of their medical records was carried out following all the standards recommended by the ethics committees in which it was approved.
Financial support and sponsorship
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
There are no conflicts of interest.
References
- Gunshot injuries in children served by emergency services. Pediatrics. 2013;132:862-70.
- [CrossRef] [PubMed] [Google Scholar]
- Social withdrawal and violence-newtown, connecticut. N Engl J Med. 2013;368:399-401.
- [CrossRef] [PubMed] [Google Scholar]
- Homicídios na Adolescencia no Brasil: IHA 2014. 2017. Rio de Janeiro: IHA. (1st ed). Available from: http://www.prvl.org.br/wp-content/uploads/2017/06/iha-2014.pdf [Last accessed on 2020 Jun 20]
- [Google Scholar]
- Ferimento por arma branca : Perfil epidemiológico dos atendimentos em um pronto socorro. Rev Rene. 2011;12:669-77. Available from: http://www.periodicos.ufc.br/rene/article/viewFile/4312/3316 [Last accessed on 2020 Jun 20]
- [Google Scholar]
- 2014. Desafios à Trajetória Profissional dos Jovens Brasileiros. Rio de Janeiro: Ipea; :267-90. Available from: http://www.ipea.gov.br/portal/images/stories/PDFs/livros/livros/livro_desafios_completo-web.pdf [Last accessed on 2020 Jun 20]
- [Google Scholar]
- Atlas da Violência 2017. 2017. Rio de Janeiro. Available from: http://www.ipea.gov.br/atlasviolencia/arquivos/downloads/8623-170602atlasdaviolencia2017.pdf [Last accessed on 2020 Jun 20]
- [Google Scholar]
- Lesões provocadas por armas de fogo atendidas em serviços de urgência e emergência brasileiros. Cien Saude Colet. 2017;22:2851-60. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232017002902851&lng=pt&tlng=pt [Last accessed on 2020 Jun 20]
- [CrossRef] [PubMed] [Google Scholar]
- Violências e direitos humanos em pesquisa com crianças. Educ Pesqui. 2015;41:1569-83. Available from: http://www.scielo.br/pdf/ep/v41nspe/1517-9702-ep-41-spe-1569.pdf [Last accessed on 2020 Jun 20]
- [CrossRef] [Google Scholar]
- Secretaria Nacional dos Direitos da Criança e do Adolescente. 1990. Conselho Nacional dos Direitos da Criança e do Adolescente. Estatuto da Criança e do Adolescente. Available from: https://www.gov.br/mdh/pt-br/centrais-de-conteudo/crianca-e-adolescente/estatuto-da-crianca-e-do-adolescenteversao-2019.pdf [Last accessed on 2020 Jun 20]
- [Google Scholar]
- Fórum Brasileiro de Segurança Pública Anuário Brasileiro de Segurança Pública 2019. 2019. p. :206.
- [Google Scholar]
- Epidemiology of pediatric fractures presenting to emergency departments in the United States. J Pediatr Orthop. 2016;36:45-8.
- [CrossRef] [PubMed] [Google Scholar]
- Violence against women, children, and adolescents during the COVID-19 pandemic: Overview, contributing factors, and mitigating measures. Cad Saude Publica. 2020;36:74420.
- [CrossRef] [PubMed] [Google Scholar]




