Translate this page into:
Clinical and imaging features of pedal macrodystrophia lipomatosa in two children with differential diagnosis review
2 Department of Orthopaedic Surgery, Division of Pediatric Orthopaedics, Faculty of Medicine, Ain-Shams University, Abbasia, Cairo, Egypt
3 Center of Medical Genetics, Division of Musculoskeletal Radiology, Faculty of Medicine, Ain-Shams University, Abbasia, Cairo, Egypt
4 Department of Radiology, Division of Musculoskeletal Radiology, Faculty of Medicine, Ain-Shams University, Abbasia, Cairo, Egypt
Corresponding Author:
Nermine S Elsayed
Center of Medical Genetics, Faculty of Medicine, Ain.Shams University, Abbasia, Cairo
Egypt
mnnrkm@gmail.com
| How to cite this article: Abdulhady H, El-Sobky TA, Elsayed NS, Sakr HM. Clinical and imaging features of pedal macrodystrophia lipomatosa in two children with differential diagnosis review. J Musculoskelet Surg Res 2018;2:130-134 |
Abstract
Macrodystrophia lipomatosa (ML) is a rare nonhereditary congenital/developmental disorder. It can manifest in limb overgrowth and disfigurement. In consequence, considerable esthetic and functional implications can develop. To overcome such problems, debulking surgery and digit amputation have been practiced. The diagnosis of ML is largely based on accurate clinical assessment and supplementary imaging modalities. The differential diagnosis of an overgrown limb(s) including ML offers numerous challenges in terms of overlapping clinical features and diversity of prognosis of the involved disorders. This study aims to describe the clinical and radiologic characteristics of two girls with ML of the foot. In particular, we intend to explore the role of magnetic resonance imaging (MRI) in clarifying the pathology and supporting the diagnosis. This study demonstrates that accurate history taking and clinical examination provide a valuable key to the diagnosis of foot ML. We used MRI effectively to delineate the characteristics of ML and confirm the diagnosis. Review of the differential diagnosis suggests a potential and important role for magnetic resonance imaging in the differential diagnosis of overgrowth disorders.Introduction
The term overgrowth in itself refers to disorders in which somatic cellular hypertrophy and/or proliferation results in either overall increase in linear growth (tall stature) or various degrees of localized tissue overgrowth/gigantism.[1],[2] Overgrowth syndromes manifest in clinically and radiologically diverse features and exhibit various degrees of musculoskeletal distortions. In general, overgrowth syndromes can be associated with craniofacial dysmorphism, mental retardation, visceral manifestations, and increased risk for acquiring particular malignancies.[2],[3],[4] Macrodystrophia lipomatosa (ML) or localized gigantism is a rare nonhereditary developmental disorder characterized by abundant fibrofatty tissue infiltration of a part or an entire extremity. Nevertheless, all components of mesenchymal tissues can be involved including muscles, periosteum, and even bone marrow. ML results in a focal or regionalized tissue overgrowth without an abnormal tall stature.[5],[6],[7],[8] ML exhibits a slight male predilection.[1] Most patients with ML present during childhood and adolescence although no age group is immune.[1] Around 115 cases of ML have been published since 1950 based on a PubMed search only.[1] ML has a tendency to involve a localized region of a limb (foot or hand) unilaterally and is usually painless.[1],[9] Less commonly, an entire upper or lower limb may be involved.[1] The lower limbs are involved in approximately 60% of cases.[1] Gross disfigurement and functional disability can complicate ML.[10],[11],[12] Surgery in the form of localized amputations or debulking has been practiced in a considerable percentage of patients for functional and esthetic reasons.[1] The invasive histopathological examination was a long-established diagnostic tool for patients with ML. Various imaging modalities have been used in the diagnostic process of ML, namely plain radiography, ultrasound, computed tomography (CT) scan,[10] and magnetic resonance imaging (MRI).[1],[13],[14] MRI is an important supplement to the diagnostic process of ML. It has been employed to portray the distinctive features of ML.[1],[6],[15],[16] MRI is also important to surgical planning.[1],[17] This study is intended to describe the clinical characteristics of two girls with ML of the foot and detail the MRI features of one of them. Our secondary aim is to highlight the differential diagnosis of ML. The authors have obtained the patient's informed written consent for publication of the study. Ethical committee approval was obtained.
Case Reports
Case 1
An 11-year-old girl presented to our institution complaining of a painless swelling of the left foot. The swelling has first been recognized in infancy but intensified recently and started to cause gait discomfort. The patient was subjected to amputation of the left second toe a few years ago due to gross deformation. She was a product of a nonconsanguineous marriage. The parents reported that their daughter's uncle suffers from multiple bilateral focal limb distortions, but no documented diagnosis has been provided. Otherwise, the family history was unremarkable. We reported no history suggestive of other system affection. The left foot swelling was not tender. We detected no other musculoskeletal abnormalities. Neurologic examination and foot perfusion were unremarkable. The clinical appearance and plain radiographs of both feet are shown in [Figure - 1]. At 6-month follow-up, the mentioned swelling of the big toe of the left foot showed an increase in size. MRI of the left foot was performed to delineate the nature of overgrown tissues and assess the extent of pathology. The technique of examination included sagittal short-tau inversion recovery (STIR) and T2-weighted images, axial T1, STIR, and T2-weighted images, coronal STIR and T2-weighted images [Figure - 2], [Figure - 3], [Figure - 4]. In general, MRI revealed abundant partially encapsulated fibrofatty tissue that was detectable in all pulse sequences. This abundant fat demonstrated signal intensity similar to that of adjoining normal subcutaneous fat. The MRI appearance of musculoligamentous and joint surfaces was unremarkable.
![[Figure - 1]](#fig_SaudiOrthopJ_2018_2_3_130_234060_f1.jpg){kind=link}
![[Figure - 2]](#fig_SaudiOrthopJ_2018_2_3_130_234060_f2.jpg){kind=link}
![[Figure - 3]](#fig_SaudiOrthopJ_2018_2_3_130_234060_f3.jpg){kind=link}
![[Figure - 4]](#fig_SaudiOrthopJ_2018_2_3_130_234060_f4.jpg){kind=link}
 |
| Figure 1: Clinical and radiographic features of the left foot. (a and b) Note the overgrowth of the left big toe and first ray of foot together with the amputated second left toe. (c and d) Anteroposterior and lateral views. Mark the extended soft-tissue shadow around the big toe and first ray of the left foot, especially on the planter surface (arrows). The bone architecture of the foot is unaltered |
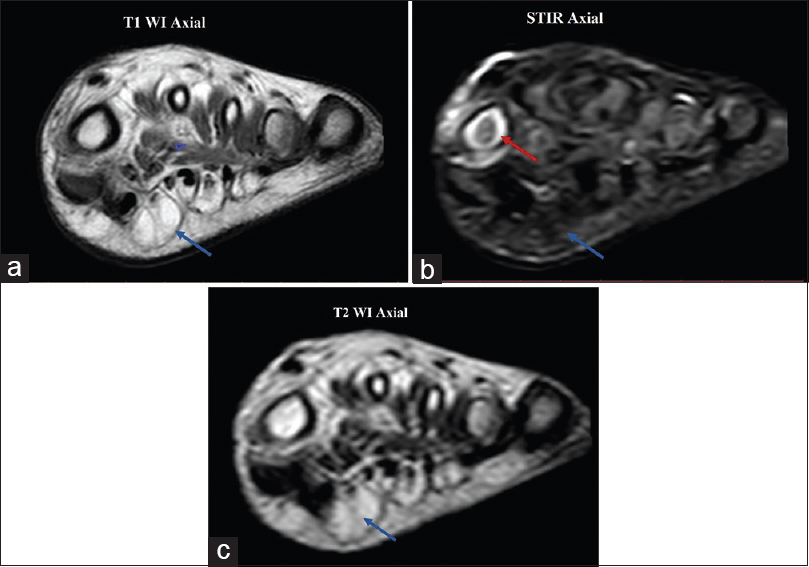 |
| Figure 2: Axial magnetic resonance imaging examination of the left foot. (a) T1-weighted axial images. Note the partially encapsulated and lobulated fatty tissue overgrowth corresponding to the plantar surface of first metatarsal (arrow) and intramuscular location of fat (triangle). It exhibits a hyperintense bright signal similar to that of surrounding subcutaneous fat. (b) short-tau inversion recovery axial images. Note the excessive fatty tissue overgrowth as previously mentioned. Fatty overgrowth exhibits a hypointense dark signal (blue arrow) similar to that of surrounding subcutaneous fat. Note the hyperintense signal of bone marrow of first metatarsal signifying edema (red arrow). (c) T2-weighted axial shows the same findings as in (a). Note that the lesion (arrow) follows the signal of fat in the subcutaneous tissue as seen in T1-weighted images |
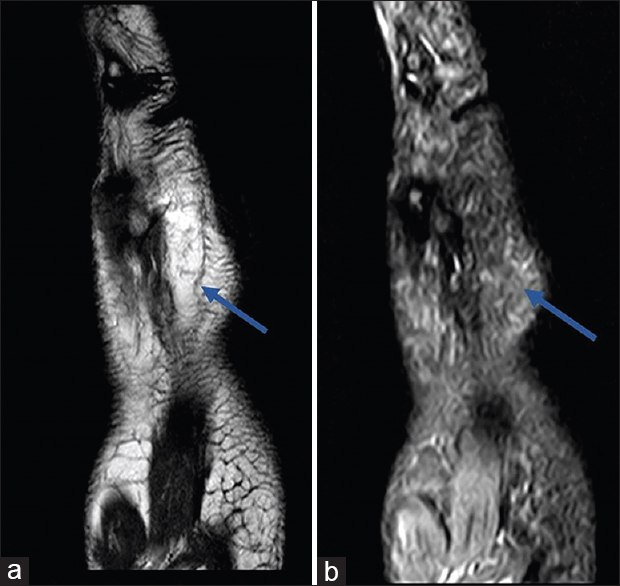 |
| Figure 3: Sagittal magnetic resonance imaging examination of left foot. (a) T2-weighted and (b) short-tau inversion recovery sagittal images show fatty overgrowth in relation to planter aspect of first metatarsal and big toe. The fatty overgrowth exhibits an intermediate and hypointense signal in (a) and (b), respectively |
 |
| Figure 4: Sagittal magnetic resonance imaging examination of the left foot. (a) T2-weighted and (b) short-tau inversion recovery sagittal images show the same fatty overgrowth (blue arrows) as in abovementioned images. (b) short-tau inversion recovery images also show bone marrow edema along medial cuneiform, navicular, and head talus (red arrows) |
Case 2
An 8-year-old girl presented to our institution complaining of a painless swelling of the left foot with deformity of the first and second toes. The condition has first been noticed shortly after birth and ran a stationary course since. The patient was subjected to a debulking and corrective orthopedic procedure of the left second toe at 4 years of age. The operation improved the foot appearance. The child accommodated for the residual deformity by wearing oversized foot wear. She was a product of a nonconsanguineous marriage. The family history was unremarkable. We reported no history suggestive of other system affection. The left foot swelling was not tender. We detected no other musculoskeletal abnormalities. Neurologic examination and foot perfusion were unremarkable. The clinical appearance of both feet is shown in [Figure - 5]. The plain radiographs were unremarkable except for regular bony expansion. The patient was unavailable for an MRI study of the feet.
![[Figure - 5]](#fig_SaudiOrthopJ_2018_2_3_130_234060_f5.jpg){kind=link}
 |
| Figure 5: Clinical features of the second child. (a and b) Note the elongated left foot with overgrown greater and second toes and residual angulation of the second toe despite debulking surgery and corrective osteotomy |
Discussion
In cases of ML, accurate history taking and clinical assessment are indispensable to the diagnostic process. This is usually supplemented by one or more imaging modality depending on the clinical scenario and availability of imaging tools.[1],[6] Nonetheless, the diagnosis of ML has historically relied on the invasive histopathologic examination.[1],[11] We believe that histopathologic examination is not routinely needed in the diagnostic process of ML, but there may be room for it in research work. Generally speaking, the concept of radiologic-pathologic correlation has been shown to enhance the diagnostic accuracy and widen the physician's interpretation of the abnormal radiologic phenomena.[18],[19] Radiologic-pathologic correlation is a long-established practice in oncologic surgery.[19] It has also been applied into practice in the field of congenital disorders such as ML[1],[11],[17] and unusual infections such as fungal osteomyelitis[18] since mass tissue resection/amputation is performed occasionally as part of the surgical management of these disorders. In our two cases, the diagnosis was readily established through an accurate clinical examination that was supplemented by a radiographic and detailed MRI assessment in the first case. Hence, we estimated that a histopathologic examination was unnecessary. A large review article showed that ML had a great predilection in favor of the involvement of a hand or foot rather than an entire upper or lower extremity, usually unilaterally.[1] Furthermore, two-digit affection is a common pattern of involvement in ML.[1] The clinical pattern of involvement in our two cases goes strictly in line with the previous findings. Numerous publications regard MRI as a useful tool for the diagnosis of ML.[1],[6],[16],[20] In the current study, we were fairly comprehensive in our coverage of all relevant aspects of MRI examination, especially the addition of STIR images. We assume that the presence of bone marrow edema along the medial side of the forefoot and midfoot found in STIR images of our first case is an early sign of a bone involvement seen in ML. It is widely acknowledged that in ML, the predominantly affected mesenchymal-derived cells are adipocytes.[1],[13],[21] The MRI features reported in our study corroborate these findings. MRI can be utilized to plan surgery particularly in regard to the visualization of median nerve infiltration, a frequent finding in ML of the hand.[17],[22],[23] In our cases, there was no justification for foot surgery neither in the first case nor for revision surgery in the second case. Besides, we found no plantar nerve affection. The presence of destructive osteoarticular changes in ML has been demonstrated even in young adults.[1],[10],[24] In our cases, we reported no destructive osteoarticular changes neither on plain radiographs nor on MRI. This may in part be related to the age factor, especially with respect to the occurrence of arthritic changes. We thought that CT scan was marginal to the diagnostic process as the patient's plain radiographs showed undisturbed bone architecture.
We decided to manage our cases conservatively because they were not significantly symptomatic. In addition, we assumed that any surgical intervention (debulking procedure) in this prepubertal stage would yield unpredictable results. We were specifically concerned about the risk of recurrence in an age era that is inherently associated with high cellular turnover. This viewpoint conforms to the management algorithm of a large review article on ML.[1]
Differential diagnosis
Differential diagnoses of ML include fibrolipomatous hamartoma,[23] neurofibromatosis Type 1,[25] Proteus syndrome,[26] Klippel—Trenaunay—Weber syndrome,[27] and hemangiomas.[28]
Fibrolipomatous hamartoma commonly occurs in association with ML of the hand.[14],[15],[17],[29],[30],[31] A typical pattern of involvement includes enlargement of the median nerve beneath the carpal tunnel and affection of its nerve territory with fibrofatty tissue infiltration. Macrodactyly and symptoms related to median nerve dysfunction are the usual presenting symptoms. Less commonly, the ulnar verve territory can be involved.[32] A detailed neuro-orthopedic hand examination and MRI can ascertain the diagnosis in most cases. In our two cases, the hand was not involved and plantar nerves of the big toe were intact.
Neurofibromatosis Type 1 also known as Von Recklinghausen's disease is a genetically determined overgrowth syndrome that is usually present in childhood. The presence of multiple café-au-lait cutaneous patches and multiple cutaneous or subcutaneous neurofibromas is highly unique to Neurofibromatosis Type 1. The presence of any of the abovementioned manifestations plus a positive family history is confirmatory.[25] Neurofibromatosis Type 1 can lead to a significant limb disfigurement, especially in association with plexiform neurofibromas, a pathognomonic but less common feature of Neurofibromatosis Type 1. Underlying skeletal changes may include kyphoscoliosis and tibial pseudoarthrosis.[25],[33] MRI can be valuable in delineating number and deeper extent of superficial plexiform neurofibromas. On T2-weighted MRI, the presence of a localized lesion with low-signal intensity centrally and a high-signal intensity peripherally is pathognomonic for Neurofibromatosis Type 1, although not a universal sign.[25],[33] The absence of café-au-lait cutaneous patches, neurofibromas, and restriction of manifestations to the left foot in our two cases argues for ML.
Proteus syndrome is another overgrowth syndrome that has a genetic background. It is characterized by sudden and rapidly progressive generalized overgrowth that is typically noticed between the 2nd and 3rd year of life.[26],[34] The overgrowth is often bilateral, asymmetrical with characteristic periarticular distortions, and occasional scoliotic curves.[26],[34] Proteus syndrome exhibits highly unique radioclinical musculoskeletal features.[26] In our two cases, the absence of bilateralism, abnormal tall stature, and limb length discrepancy lends support to the diagnosis of ML.
Klippel—Trenaunay syndrome and Parkes Weber syndrome are rare overgrowth syndromes that manifest in lower limb hypertrophy and length discrepancy. They comprise capillary/venous malformations in association with soft-tissue or bony overgrowth and are usually recognizable at birth. They are occasionally referred to as one disease entity, namely Klippel—Trenaunay—Weber syndrome.[27] Nonetheless, Parkes Weber syndrome is characterized by fast-flow vascular malformations, which may impact negatively on orthopedic interventions and debulking surgery.[27],[35] MRI can assist in delineating the nature of the hypertrophied soft tissues and bone pathology. Magnetic resonance angiography can aid in detecting vascular malformations, especially in the preoperative setting.[27] In our two cases, the absence of both soft-tissue vascular malformations and limb length discrepancy favors the diagnosis of ML.
Hemangiomas also known as infantile hemangioma usually present in infancy with red or bluish patches that may be flat or elevated. Their clinical behavior is characterized by a period of rapid growth followed by spontaneous regression usually before 5 years of age.[28] If the diagnosis is unsettled, ultrasound or MRI can be beneficial. On MRI, during growth phase, hemangiomas exhibit a well-delineated lobulated lesion with low/intermediate and high-signal intensity on T1-weighted and T2-weighted images, respectively. On gadolinium contrast-enhanced MRI, proliferating hemangiomas are characterized by early, diffuse, and uniform enhancement with flow voids. During the involution phase, hemangiomas exhibit a more heterogeneous appearance with foci of high-signal intensity on T1-weighted images due to gradual fat replacement.[28] Although the foot hypertrophy in our two cases was first recognized in infancy, the absence of localized vascular skin lesions and failure of involution argue for ML.
Conclusion
This study demonstrates that meticulous history taking and clinical examination are crucial contributors to the diagnosis of ML. In that regard, a detailed history relating to the overgrown limb(s) and a comprehensive orthopedic examination is of particular importance. The study suggests a potential and important role for MRI in regard to delineating the characteristics of ML and the differential diagnosis of overgrowth disorders. This study underscores the importance of a multidisciplinary approach to such a rare disorder.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the parents have given their consent for their children's images and other clinical information to be reported in the journal. The parents understand that names and initials of the patients will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Authors contributions
NS and HA conceived and designed the study. TAE and HS performed acquisition, analysis, and interpretation of data. TAE wrote the draft of the article. All authors have reviewed it critically for important intellectual content, have checked the article for plagiarism, and are responsible for the content and similarity index of the manuscript. Finally, all authors approved the version to be published.
| 1. | Prasetyono TO, Hanafi E, Astriana W. A review of macrodystrophia lipomatosa: Revisitation. Arch Plast Surg 2015;42:391-406. [Google Scholar] |
| 2. | Lacerda Lda S, Alves UD, Zanier JF, Machado DC, Camilo GB, Lopes AJ, et al. Differential diagnoses of overgrowth syndromes: The most important clinical and radiological disease manifestations. Radiol Res Pract 2014;2014:947451. [Google Scholar] |
| 3. | Edmondson AC, Kalish JM. Overgrowth syndromes. J Pediatr Genet 2015;4:136-43. [Google Scholar] |
| 4. | Ko JM. Genetic syndromes associated with overgrowth in childhood. Ann Pediatr Endocrinol Metab 2013;18:101-5. [Google Scholar] |
| 5. | Çelebi F, Karagulle K, Oner AY. Macrodystrophia lipomatosa of the foot: A case report. Oncol Lett 2015;10:951-3. [Google Scholar] |
| 6. | Kwon JH, Lim SY, Lim HS. Macrodystrophia lipomatosa. Arch Plast Surg 2013;40:270-2. [Google Scholar] |
| 7. | Khan RA, Wahab S, Ahmad I, Chana RS. Macrodystrophia lipomatosa: Four case reports. Ital J Pediatr 2010;36:69. [Google Scholar] |
| 8. | Pandey AK. Magnetic resonance imaging of a case of monomelic macrodystrophia lipomatosa. Australas Radiol 2007;51 (Suppl 4):B227-30. [Google Scholar] |
| 9. | Durairaj AR, Mahipathy SR. Macrodystrophia lipomatosa of the toe: A rare case report. J Clin Diagn Res 2016;10:PD27-8. [Google Scholar] |
| 10. | Sharma R, Gupta P, Mahajan M, Arora M, Gupta A. X-ray and computed tomography findings in macrodystrophia lipomatosa of the foot with secondary osteoarthritic changes diagnosed in an elderly female: A case report. Radiol Bras 2017;50:132-4. [Google Scholar] |
| 11. | Majumdar B, Jain A, Sen D, Bala S, Mishra P, Sen S, et al. Macrodystrophia lipomatosa: Review of clinico-radio-histopathological features. Indian Dermatol Online J 2016;7:293-6. [Google Scholar] |
| 12. | Maheswari SU, Sampath V, Ramesh A, Manoharan K. Macrodystrophia lipomatosa: An unusual cause of localized gigantism. Indian J Dermatol 2016;61:347. [Google Scholar] |
| 13. | Burt AM, Huang BK. Imaging review of lipomatous musculoskeletal lesions. SICOT J 2017;3:34. [Google Scholar] |
| 14. | Boren WL, Henry RE Jr., Wintch K. MR diagnosis of fibrolipomatous hamartoma of nerve: Association with nerve territory-oriented macrodactyly (macrodystrophia lipomatosa). Skeletal Radiol 1995;24:296-7. [Google Scholar] |
| 15. | Shekhani HN, Hanna T, Johnson JO. Lipofibromatous hamartoma of the median nerve: A case report. J Radiol Case Rep 2016;10:1-7. [Google Scholar] |
| 16. | Singla V, Virmani V, Tuli P, Singh P, Khandelwal N. Case report: Macrodystrophia lipomatosa-illustration of two cases. Indian J Radiol Imaging 2008;18:298-301. [Google Scholar] |
| 17. | Brodwater BK, Major NM, Goldner RD, Layfield LJ. Macrodystrophia lipomatosa with associated fibrolipomatous hamartoma of the median nerve. Pediatr Surg Int 2000;16:216-8. [Google Scholar] |
| 18. | El-Sobky TA, Haleem JF, Samir S. Eumycetoma osteomyelitis of the calcaneus in a child: A radiologic-pathologic correlation following total calcanectomy. Case Rep Pathol 2015;2015:129020. [Google Scholar] |
| 19. | Davies AM, Mangham DC. Bone tumors. In: Gourtsoyiannis NC, Ros PR, editors. Radiologic-Pathologic Correlations from Head to Toe: Understanding the Manifestations of Disease. Berlin, Germany: Springer; 2005. p. 661-80. [Google Scholar] |
| 20. | Wang YC, Jeng CM, Marcantonio DR, Resnick D. Macrodystrophia lipomatosa. MR imaging in three patients. Clin Imaging 1997;21:323-7. [Google Scholar] |
| 21. | Van den Heever AJ. Macrodystrophia lipomatosa. Afr J Radiol 2014;18:4. [Google Scholar] |
| 22. | Cerrato F, Eberlin KR, Waters P, Upton J, Taghinia A, Labow BI, et al. Presentation and treatment of macrodactyly in children. J Hand Surg Am 2013;38:2112-23. [Google Scholar] |
| 23. | Tahiri Y, Xu L, Kanevsky J, Luc M. Lipofibromatous hamartoma of the median nerve: A comprehensive review and systematic approach to evaluation, diagnosis, and treatment. J Hand Surg Am 2013;38:2055-67. [Google Scholar] |
| 24. | Faizan M, Ahmed S, Khalid S, Zahid M. Localized gigantism. Saudi Med J 2015;36:762-3. [Google Scholar] |
| 25. | Friedman JM. Neurofibromatosis 1. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Bean LJH, Stephens K, et al., editors. GeneReviews®. Seattle (WA): University of Washington, Seattle; 1993-2017; 1998. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1109/. [Last updated on 2014 Sep 04]. [Google Scholar] |
| 26. | El-Sobky TA, Elsayed SM, El Mikkawy DM. Orthopaedic manifestations of proteus syndrome in a child with literature update. Bone Rep 2015;3:104-8. [Google Scholar] |
| 27. | Sung HM, Chung HY, Lee SJ, Lee JM, Huh S, Lee JW, et al. Clinical experience of the Klippel-Trenaunay syndrome. Arch Plast Surg 2015;42:552-8. [Google Scholar] |
| 28. | Nguyen TA, Krakowski AC, Naheedy JH, Kruk PG, Friedlander SF. Imaging pediatric vascular lesions. J Clin Aesthet Dermatol 2015;8:27-41. [Google Scholar] |
| 29. | Senger JL, Classen D, Bruce G, Kanthan R. Fibrolipomatous hamartoma of the median nerve: A cause of acute bilateral carpal tunnel syndrome in a three-year-old child: A case report and comprehensive literature review. Plast Surg (Oakv) 2014;22:201-6. [Google Scholar] |
| 30. | Yesilada AK, Sevim KZ, Sucu DO, Dagdelen D, Sakiz D, Basak M, et al. Combined triggering at the wrist and fingers and severe carpal tunnel syndrome caused by macrodystrophia lipomatosa. Case report and review of literature. Acta Chir Plast 2013;55:23-5. [Google Scholar] |
| 31. | van der Meer S, Nicolai JP, Meek MF. Macrodystrophia lipomatosa: Macrodactyly related to affected nerves, and a review of the literature. Handchir Mikrochir Plast Chir 2007;39:414-7. [Google Scholar] |
| 32. | Siddiqui MA, Ahmad M, Redhu N, Ahmad I, Ullah E. Macrodystrophia lipomatosa with ulnar distribution in hand: MR evaluation of a rare disorder. JBR-BTR 2015;98:43-4. [Google Scholar] |
| 33. | Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. AJR Am J Roentgenol 2012;199:W99-106. [Google Scholar] |
| 34. | Cohen MM Jr. Proteus syndrome review: Molecular, clinical, and pathologic features. Clin Genet 2014;85:111-9. [Google Scholar] |
| 35. | Kulungowski AM, Fishman SJ. Management of combined vascular malformations. Clin Plast Surg 2011;38:107-20. [Google Scholar] |
Fulltext Views
4,480
PDF downloads
1,789




